Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Home.netspeed.com.au
The PBS Panic – the consumer perspective
Ian McAuley, University of Canberra, onbehalf of the Australian Consumers’Association. Paper for the 3rd Annual “Future of the Pharmaceutical Benefits Scheme Conference”, Informa Conferences, 24th & 25th August 2005. Abstract
Concerns about PBS expenditure are m isplaced,because they are from a narrow fiscal perspective,that fails to consider the total cost ofpharm aceuticals, the benefits of pharm aceuticals, orthe context of pharm aceuticals in health caredelivery.
Pharm aceuticals are but one input into health careprogram s. Health program s need to be re-arrangedaround consum er, rather than provider divisions.
W hen governm ents seek to contain publicexpenditure by raising co-paym ent thresholds theydo not im prove econom ic resource allocation. Rather, they leave consum ers dependent on a highlyprotected retail pharm acy industry shielded fromcom petition. The Australian Consumers’ Association
The Australian Consumers’ Association (ACA) is a non-profit, non-party-politicalorganisation. The ACA is completely independent. It is not a governmentdepartment or agency and it receives no funding from any government. Neitherdoes it receive subsidies from industry, manufacturers, unions or any other groups,and it doesn’t take advertisements in any of its printed magazines or on its website. The ACA gets its income from the sale of Choice magazine, Choice Online andother publications and products. They currently has over 145,000 subscribers totheir products.
The ACA represents and acts in consumers’ interests. It lobbies and campaigns onbehalf of consumers to promote their rights, to influence government policy, and toensure consumer issues have a high profile in the public arena.
The ACA is committed to providing information on a whole range of consumerissues including health, financial services, information technology andcommunications, travel, food and nutrition, computer technology and consumerpolicy. The PBS panic – the consumer perspective
Ian McAuley, University of Canberra, on behalf of theAustralian Consum ers’ Association
It is almost an article of public policy faith that the PBS is a large and unsustainable burdenon our community. The title of this conference is “funding and sustainability”; I doubt if aconference on the banking or auto industry would include the term “sustainability”. Yet onecan be reasonably confident that in twenty or fifty years time we will still be buying and usingpharmaceuticals. Similarly, there is a session titled “blow out”, but when, for example, salesof DVDs grow exponentially, do we refer to a “blow out” or do we refer, rather to marketingand technological success?
Underlying some of this terminology perhaps is an assumption that any growing area ofpublic expenditure constitutes a problem (unless it happens to be national security). Thatnarrow assumption dominates thinking in the Commonwealth Treasury Department, whovalue fiscal stringency ahead of sound economic policy.
In this session I want to make two points relating to consumer interests. First, the view thatgrowing public expenditure constitutes a problem is not one shared by the ACA. That is notto suggest the ACA has an irresponsible “tax and spend” attitude to public finance; rather thepoint is that this view reflects a narrow understanding of the issue. Second, if we are tocontrol pharmaceutical expenditure without compromising benefits, we need the functioningof either strong markets or strong government. The way most health programs are structured,however, provides consumers with neither form of protection against exploitation andresource misallocation. Reframing – a world without the PBS
Most consumers most of the time would not have much concern with the PBS, because theyhave little interaction with health care providers. The use of health services is heavilyskewed; most of us have the good fortune of needing very little by way of health care. In anyone year 20 percent of the population have no Medicare claims at all; a further 31 percenthave between one and five claims a year. While we don’t have figures on the distribution ofPBS claims, it is safe to suggest that most people will not be in families eligible for the PBSsafety net provisions – a point to which we return later.
Most consumers’ interests lie in knowing that they have available high quality and affordablehealth care when they need it. When people do need health care, however, they confront aconfusing array of fragmented programs. Let’s consider someone with a minor weekendsporting injury – Cathy – who seeks medical attention. Her treatment path may be:
(1) A GP consultation – possibly bulk billed
(2) Diagnostic imaging – free if at a public hospital, otherwise reimbursable up to 85
percent of the Medicare Schedule Fee, and with an open-ended top-up payment;
(3) A specialist consultation – reimbursable up to 85 percent of the Medicare Schedule
Fee, and with an open-ended top-up payment;
(4) Dressings and drugs, some of which may be Schedule 2 or 3 pharmaceuticals with
no Commonwealth support, some of which may be prescription pharmaceuticalswith PBS subsidies – a capped co-payment. She may be in luck and find thepharmacy is not too far from her GP, but to find one open is a challenge, forpharmacy opening hours are generally designed for the convenience of their older,retired customers, without work commitments.
(5) Standard analgesics available from a supermarket;
(6) Physiotherapy – with no government support, but with some limited reimbursement
if he or she is part of the minority (43 percent) of Australians with privateinsurance.
Unless she is willing to wait in a public hospital casualty room, she probably has to wait untilMonday even to make an appointment. She will spend much of her time waiting in line, andsome of that time filling in forms, in longhand, repeating her name, address and other basicdetails. (Someone else will transcribe this into unlinked databases, with possibilities for errorall along the way.)
That’s without mentioning Cathy’s possible eligibility for safety nets, which have differentcriteria for different services, and without her possible need for hospitalization. There aretwo safety nets for medical services, for example – a gap safety net and a general safety net,one calculated on individual payments and the other on family payments. There is a taxrebate for uninsured medical expenses above $1500. The consumer has one need, and severaldifferent payment systems.
To see the full absurdity of this situation, imagine if, when your car develops minormechanical trouble, you had to go to one place for a diagnosis, another for parts, another forsome repairs, another for some other repairs, with different bills from each provider – andwith the complication of having to drive around in a defective vehicle to obtain all theseparts. Not even the Soviet bureaucracy, in all its bureaucratic glory, managed to impose sucha system on consumers.
Yet we persist with an antiquated structure of health care programs. Program divisions arebased on providers’ demarcations, rather than consumers’ needs. This set of divisionsdetermines the perspectives the policy elites, such as Treasury bureaucrats, bring to bear onhealth care. As an example, the following is one of the key tables from the Commonwealth’sIntergenerational Report:
Table 1. Projected Commonwealth health spending, by components (per cent of GDP) All health
Source: From Table 9, Intergenerational Report (Health component only shown)
The most striking feature of that table may be its alarmist projections, but there are two otheraspects that are not so obvious – its confinement to fiscal projections and its confinement toone input to health care.
To deal with the alarmist projections first. Simply looking at the PBS, we see it as the fastestgrowing component of health outlays, rising from 0.60 percent of GDP to 3.35 percent ofGDP, over 40 years. There is an air of panic in the Intergenerational Report.
But let’s look at this projection. We can reasonably expect a rising GDP over the next 40years, and, with a little straightforward mathematics, can show that if we achieve just 0.07percent annual growth in per-capita GDP, we can afford even these high outlays withouthaving to transfer resources from any other activity.1 Even the Treasury projections are easilyaffordable. And it’s surprising, given the scale economies in pharmaceutical manufacture,that the Treasury modelling does not assume real price falls as volumes rise; are theyassuming the Australian Government lacks the power to negotiate price/volume agremeentsin the PBS? Are they assuming that the power of pharmaceutical companies’ advertisingbudgets will be overwhelming?
Another feature of this table is that it is presented only in terms of the fiscal costs of the PBS. It is a financial projection, not an economic projection. An economic projection wouldinclude all costs of pharmaceuticals, be they incurred through Commonwealth outlays, stategovernment outlays, or private outlays. And it would include some estimate of benefits;indeed if the benefits of pharmaceuticals did not exceed their costs there would be somethingseriously wrong.
In fact the Commonwealth accounts for only one half of our expenditure on pharmaceuticals. A more comprehensive table would be of the form shown below in Table 2. If thebureaucrats who prepare the Intergenerational Report were concerned with our outlays onpharmaceuticals, rather than on fiscal bookkeeping, they would gather the data to completethe table shown below. Then, at least, we might see how much our pharmaceuticalexpenditure is projected to grow.
If per-capita GDP grows by just 2.845 percent over 40 years, we could devote 3.35 percent of GDP to thePBS. That requires a growth rate of only 0.07%
Table 2. Expenditure on pharmaceuticals (per cent of GDP)
Source: AIHW Health Expenditure Bulletins and ABS GDP estimates
This table, while including individual outlays, still does not include any estimate of thebenefits of pharmaceuticals. Furthermore it doesn’t include purchases by state governmentsfor hospital pharmaceuticals.
It is meaningless to talk about “affordability” or “blow outs” in isolation – any more than itmakes sense to talk about affordability and blow outs in expenditure on DVDs or carrots. Wechoose to buy pharmaceuticals, either collectively through public budgets or individuallythrough our own pockets, because we perceive pharmaceuticals to be beneficial. FortunatelyAustralia, in the rigorous cost-benefit processes used by the PBAC, has a means of ensuringwe do spend our pharmaceutical budgets wisely. (It’s unfortunate that such a disciplinedcost-benefit approach used by the PBAC does not extend across the whole of health policy; ifit did there could be great potential for cost savings, particularly in the area of public andcommunity health.)
What the Commonwealth, particularly the Treasury Department, seems to be concerned withis not whether we are spending too much or too little on pharmaceuticals – which wouldrequire a proper economic analysis. Rather, its concern seems to be purely with budgetaryoutlays, as if there is something intrinsically undesirable in tax-funded programs.2
There is a strong case for collective funding of some or all of our health costs; a large body ofevidence suggests that price considerations deter consumers from early intervention in healthproblems, leading to much more expensive interventions as their problems worsen. Andthere are equity and social insurance reasons why people choose to share health care coststhrough public budgets. There are also reasons for using market signals in some aspects ofhealth care, but, as we will see further on in this paper, our Commonwealth and stategovernments have effectively muzzled market forces in retail pharmacy.
When the Commonwealth economizes on PBS expenditure by lifting safety net thresholds orintroducing special patient contributions they do not improve economic resource allocation,because they are transferring expenditure into a highly distorted market – a market which hasbeen distorted by deliberate government intervention.
For an illustration of the conflicts that can occur between Treasury and Health Departments, see SteveLewis “Health cuts bad: Abbott” The Australian 10 August 2005. Lewis’s article suggests that healthM inister Abbott is in conflict with the Treasurer’s desire to cut health spending to protect the budget,arguing that health programs represent an investment in a richer and more productive society.
The final and more serious limitation of the Commonwealth perspective is that it narrowlyfocuses on pharmaceuticals. But pharmaceutical therapies are part of health care; they do notstand apart. We can note even from the Commonwealth’s own table that other componentsof health care are rising less steeply than pharmaceuticals.
Our injured weekend athlete, Cathy, shouldn’t have to be concerned with separategovernment programs such as the PBS or Medicare. She has an injury and seeks cure oramelioration. She is concerned that she gets value for money, either through co-payments orher taxes. To return to our car service analogy, we are usually more concerned with our totalbill rather than its components – labour, lubricants, electrical parts etc. If, over ten or twentyyears, we found that the cost of parts had risen strongly while the cost of labour had fallen, wewould accept the benefit of this substitution, and not get too concerned because onecomponent had risen in price.
In health care our governments’ program structures are flawed. They are structured aroundinputs (pharmaceuticals, medical services, hospitals), rather than consumers. There are manyways a consumer-based program structure may be designed. For example, just as mostcorporations structure their divisions around their customers, we could consider threeconsumer-based health care programs:
for those with occasional needs – most consumers most of the time;
for those with ongoing needs – particularly those with chronic conditions;
Alternatively, we may structure our programs around demographic groups with particularneeds – people in remote communities, adolescents, the aged etc. I will leave it to ProfessorJohn Dwyer to suggest how programs can be integrated around patients rather than providers. (That need for integration was the overwhelming theme of the 2003 Health Summit.) Forillustration, to help us re-frame our thinking, I have illustrated a possible programarrangement in a simplified matrix below, with the $$ signs indicating where heavyexpenditure is likely to be revealed. Program s
Under such a structure, integrated around consumers, attention would be focussed onconsumers. Appropriations would be made to these programs (occasional care, ongoing careand acute care in this example), the administrators of which would spend money on services
(pharmaceuticals, medical, hospital), but the prime focus of public policy considerationwould be on costs and benefits of these consumer-based programs. As a secondaryconsideration there may be some consolidation of reporting down the matrix, for example,pharmaceutical expenditure. Treasury would still have its eye on the figures, but its attentionwould no longer be on inputs by type; it would be concerned with public and privateresources devoted to consumer-based programs, and to their outputs and outcomes.
Of course such a rearrangement would be difficult within the present structure ofCommonwealth/State responsibilities, but I’m sure John Dwyer will convince us that thesebarriers can be broken down. Even within the Commonwealth there could be far moreintegration of services. With all the power the Commonwealth has over the location ofpharmacies, for example, it is extraordinary to see that there are still impediments to physicalintegration of pharmacies with medical clinics.
Would this be the end of the PBS? In name, yes, but it would still be possible to retain thePBAC and the PBPA – they are the bodies giving the scheme its purchasing strength.
Let’s return to Cathy. If she incurs her injury once we have a more consumer-friendlyprogram structure, she should be able to get all her services under one roof, with one bill, andone safety net, one set of records. If that one roof is large enough it may cover enough GPs to sustain a basic weekend roster, with a full diagnosis and treatment early in the workingweek. Her pharmaceutical regime may be developed in a face-to-face consultation betweenthe GP and the pharmacist – perhaps with a physiotherapist also in attendance to help her in achoice of therapies. There would be obvious administrative savings, and risk of receivingconflicting treatment would diminish. And it may be a little more rewarding for the healthcare professionals to find they are dealing with a whole episode of care – the pharmacists’knowledge, in particular, accumulated over many years of difficult study, would be put to farbetter use than it is in the task of running a corner store.
What I haven’t touched on, as yet, is whether Cathy is provided with free or charged service. I want to turn briefly to that issue. Markets or governments?
In all markets consumers are concerned with market outcomes – product price, quality,choice, safety and other attributes.
Sometimes these needs can be served in competitive markets, sometimes they can be servedin highly-regulated markets with or without public ownership. The consumer movement wasa powerful ally of those seeking to reduce Australia’s high tariffs, and has supported strongcompetition policy. The consumer movement has also been a staunch defender of food andpharmaceutical regulation and of publicly funded and publicly provided health care programs.
From a consumer perspective, retail pharmacy is in the worst of all worlds. It is neithercompetitive nor adequately regulated by governments.
As pointed out, most consumers most of the time are not covered by the Government’s safetynets; when they buy PBS pharmaceuticals they have to pay a price up to the $28.60 maximumpatient contribution. They may even have to pay more if their prescription is for a brand
name where a generic pharmaceutical is available, or when there is a therapeuticallyequivalent medication and where a special patient contribution is required.
While many will reasonably argue that the $28.60 co-payment imposes an unreasonableburden on many consumers, it does have the benefit of providing a price cap. If there are tobe co-payments in health care, from a consumer perspective capped co-payments are alwayspreferable to open-ended co-payments. (This is one of the consumer movement’s objectionsto the private health insurance support for ancillary services, which cap the insurers’ liabilitywhile leaving consumers with an open-ended risk. In fact it is a misrepresentation to call suchcover “insurance”.)
Many pharmaceuticals however, particularly those out of patent, should have a retail pricewell below $28.60. For these pharmaceuticals the consumer is left dependent on thepharmacist’s pricing decision, without the protection of either market competition orgovernment regulation.
Nicola Ballenden, former health policy officer for the Australian Consumers’ Association,described in detail common practices in relation to such pharmaceuticals. Pharmacistsroutinely charge more than the price the Commonwealth pays for similar prescriptions. Thisis in spite of the fact that sales of unsubsidised drugs are funded with immediate cashpayments – Commonwealth PBS payments are on a monthly reimbursement basis.
The items pharmacists routinely add to the Commonwealth price are a $0.95 charge forrecording the medicine for safety net purposes (even though it is the consumer’sresponsibility to manage his or her own safety net records, and most consumers don’t qualifyfor the safety net), and, to quote from Commonwealth correspondence “a further additionalpatient charge amounting to 10 percent of the maximum patient contribution ($28.60) plus 50cents (i.e. $2.86 + $0.50).”3 This is in spite of the fact that pharmacists often receive heftydiscounts from wholesalers on generic drugs – discounts they fail to pass on to consumers.4
In addition to these practices, at the time of the survey, Nicola found:
.some pharmacists appeared to be routinely charging something called a ‘furtheradditional patient charge’ on some PBS drugs. On pursuing this, ACA also foundthat certain pharmacy pricing software operated with a default setting that addedhuge mark-ups leading, ACA believes, to higher prices for consumers. The priceguide came from the Pharmacy Guild, the organisation that represents localpharmacists, and in fact one of the software companies is also part-owned by theGuild.5
Following the ACA’s intervention, which had alerted competition authorities to thesepractices, the pharmacists’ software has been changed to remove the high markups as adefault setting. But it reflects poorly on our public policy processes if it has to be left to
Correspondence from Pharmaceutical Access and Quality Branch, Department of Health and Ageing toACA, 14 January 2005.
M ark Davis “Chemists’ discounts rort under attack” Australian Financial Review 14 April 2005.
Nicola Ballenden “The pharmacy: why it can’t stay a closed shop” Consuming Interest W inter 2005.
consumer watchdogs to bring such pressure on the industry. The ACA receives nogovernment support – subscribers and members cannot claim tax deductions – and it has onehealth policy officer, whose responsibilities cover the entire health arena. By contrast theGuild, receiving generous tax-deductible support from pharmacists, has a number ofspecialized staff and immense lobbying resources. Before the 2004 federal election, forexample, the Guild mounted a massive political campaign against competition reform, aimedat ensuring they would once more receive from John Howard a “letter of comfort” – aguarantee of protection from competition – as they had received during previous campaigns.6
Lest anyone believe the Guild is partisan, it should be pointed out that most pharmacists’privileges relating to advertising, ownership and location are based on state legislation. In arare display of bipartisanship and federal cooperation, in May 2004 Prime Minister Howardand Premier Carr reaffirmed support for protection of the retail pharmacy industry.7 (As aminor token towards deregulation they did agree to lift a restriction on the number ofpharmacies an individual can own from three to five – a move that may allow a fewpharmacists to enjoy some scale economies, but which will bring no consumer benefits.)
In fact, the opportunity for exploitative pricing came about during the time of the HawkeGovernment, in a move which effectively removed Commonwealth responsibility for anyprice control on non-subsidised pharmaceuticals.
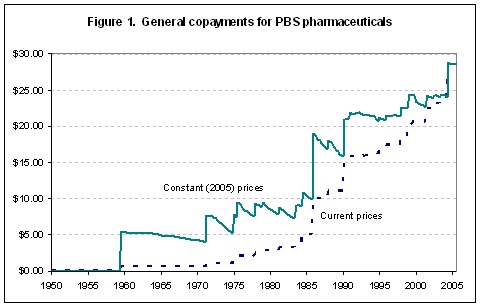
Until 1960, when a five shilling co-payment was introduced, all pharmaceuticals suppliedunder the PBS were free. The five shilling co-payment, which equates to around $5.50 in2005 prices, was hardly burdensome, and there were probably few (if any) pharmaceuticalswhich would have reasonably been priced below that level. Many of the pharmaceuticalswhich would dominate the PBS in future years were either still in patent or yet to be listed.
For the following 15 years there were a few adjustments to the co-payment. In 2005 prices, itstayed between four and eleven dollars – low enough to ensure almost all pharmaceuticals onthe PBS were subject to some Commonwealth PBS contribution and therefore effective pricecontrol.
In 1986, however, the Commonwealth raised the co-payment to $10, which, in 2005 prices, isaround $19. At the same time many pharmaceuticals were coming off patent. Manypharmaceuticals fell in real and nominal prices, so were no longer requiring a PBS subsidy. This price reduction was seldom passed on to consumers, however – pharmacists could go oncharging consumers up to the total co-payment level. The PBS had ceased to be aninstrument of price control, except for those pharmaceuticals for which a Commonwealthsubsidy is paid.
This change coincided with a fundamental shift in Commonwealth economic policy – a shiftwhich has its roots in budgetary changes in the mid eighties, and which has been extendedever since. Starting with “reforms” such as the Financial Management Improvement Programin 1988 and developing further with the Charter of Budget Honesty in 1998, theCommonwealth has largely abandoned microeconomic management in its budgetary
M ark Davis “Seeking prescription to cure competition” Australian Financial Review 17 June 2005.
Prime M inister media release “Pharmacy and National Competition Policy” 5 M ay 2004.
processes. Its concern has become a narrow financial focus on its own outlays – in this casePBS subsidies. If it can achieve budgetary savings through cost-shifting on to other parties,such as consumers, then it will do so, provided the macroeconomic effects are not too severe. In most cases it won’t even try to measure the extent of the cost-shifting; one will note, forexample, that the Commonwealth’s PBS statistics, while being extensive for subsidizedpharmaceuticals, are silent when it comes to non-subsidized prescriptions.
One may believe that a government does not wish cost-shifting to result in inflation. But lowconsumer price inflation in other areas (clothing, household goods) has tended to compensatefor health care price inflation.8
In general, under both Labor and Coalition administrations, the Commonwealth has relied oncompetition policy to achieve microeconomic reform, but retail pharmacy has managed toshield itself from national competition policy.
To justify this exemption, pharmacists like to portray themselves as “consumer friendly”,using emotive terms such as “community pharmacy”, but former ACCC Chair Alan Fels, re-frames that perception. The local pharmacy is part of a well-organized highly profitableindustry:
Australia’s 5000 pharmacies are among the most protected businesses in thecountry, wrapped in state and federal regulations that restrict their operations inalmost every conceivable way.
The states license both pharmacists and their premises, limit ownership to qualifiedpharmacists (largely precluding corporate ownership), limit the number of
From 1992 to 2003 health care inflation has been at about one percent greater than general inflation(AIHW Health Expenditure Bulletin 2002-03). Over the last five years to 2005, the gap between healthinflation and general inflation as measured by CPI components has widened to 2.3 percent.
pharmacies owned, require a pharmacist to always be in attendance, and restrictadvertising and promotion.
Canberra weighs in with another raft of controls on dispensing fees, discountprohibitions on drug prescription costs, limits on the number and location ofpharmacies (geographical monopolies) and, of course, further controls onadvertising.
Chemists provide a critical health service, and deal in dangerous drugs, so many ofthese controls are necessary. But successive inquiries have expressed concern at theanti-competitive effects of the awesome array of controls – namely, that consumerspay higher prices.
Community pharmacy in Australia is a $6 billion business with 40,000 employees. It is also very profitable. The average pharmacy operating margin is 8 per cent,several times larger than the “all retailing” average of 2 per cent.9
The retail pharmacy industry has become so used to these privileges that it seems to haveforgotten what a competitive market would look like. In a use of language that Orwell wouldclassify as Newspeak, the Pharmacy Guild claims that for pharmaceuticals priced below thepatient co-payment “market forces apply and pharmacists can compete with each other as towhat price they might charge”.10 It’s a strange idea of “market forces”, when priceadvertising is specifically prohibited, and when location regulations make it difficult forconsumers to shop around. How is a consumer to know what is a reasonable price withoutany reference point of comparative price information? How is a consumer to find, forinstance, unless he or she has a particularly friendly pharmacist, the price the Commonwealthpays for common generic pharmaceuticals – $11.28 for the contraceptive pill and $8.54 forAmoxycillin?11 If they want market forces to work, why does the Commonwealth not makethese prices readily available to consumers on a website? Where can consumers find the agreed “special patient contributions”?
What holds for PBS pharmaceuticals also holds for non-prescription pharmaceuticals inSchedule 2 (pharmacy only) and Schedule 3 (pharmacist only), and for private prescriptionsnot covered by PBS subsidies. Australians, on average, spend $400 a year on “Medicines,pharmaceutical products and therapeutic appliances” other than prescriptions, most of whichwould be spent in pharmacies.12 With private health insurance permitted to cover privateprescriptions, there is a further suppression of any market discipline on pharmacists’ pricing.
Alan Fels and Fred Brenchley “Dispense some competition to the pharmacies” Sydney M orning HeraldApril 8 2004.
Correspondence from Pharmacy Guild of Australia to the ACA, 28 January 2005.
Levonorgestrel with ethinyloestradiol 21 tablets, Ampicillin capsule 250 mg x 24, December 2004 prices.
ABS Household tables (Cat 6535.05) indicate average weekly expenditure on “M edicines, pharmaceuticalproducts and therapeutic appliances” to be $11.51, of which $3.71 is for prescription pharmaceuticals. Conclusion
I have not touched on the issue of whether pharmacies should be permitted to operate withinsupermarkets. On that delicate topic I’d suggest that it could result in useful pricecompetition and the convenience of more consumer-friendly opening hours. The retailpharmacy industry claims that the quality of professional service would be compromised, butwhen the ACA surveyed the industry in 2004 it gave the industry a less than glowing reportcard; the quality of professional advice was below the standard the ACA would have sought.13 In two thirds of the 87 pharmacies visited by ACA’s experts the quality of advice was rated as“poor”.
The short term prospects for competitive reform don’t look promising, with bipartisansupport for the status quo. The history of economic privilege suggests that it is very hard todislodge; once a group, particularly a small well-defined group, gains privilege, theyaccumulate the means to defend that privilege.
I recall a similar mythology about tariff protection, however. Tariff protection was anembedded aspect of the Australian Settlement; no government was going to demolish it. Butthat demolition occurred, from an unlikely quarter – the Hawke Government, inheritor ofLabor’s tradition of protectionism. I might add that the consumer movement supported thosepolicies strongly.
Competitive reform, however, is not in itself adequate to serve consumers’ interests. Pharmacies in supermarkets or big chains like Walgreens would still preserve a separation ofpharmacy from other aspects of health care.
We need to think more widely than the existing supply-side structures like the PBS or “retailpharmacy”, and call on governments to take the lead in redesigning our health care programsinto divisions that respond to consumer interests.
“Dispensing advice” Choice September 2004.
Ambito Disciplinare 4 e 9 – classi A043 – A050 – A051 e A052 CRITERI GENERALI 1) Pertinenza: rispondenza al quesito proposto; riferimento a costrutti teorici pertinenti; presenza di esempi contestualizzati; riferimento a eventuali sperimentazioni didattiche e/o a ricerche nazionali e internazionali; per le prove che prevedono una traduzione dal greco e dal latino viene anche valutata la pi
 processes. Its concern has become a narrow financial focus on its own outlays – in this casePBS subsidies. If it can achieve budgetary savings through cost-shifting on to other parties,such as consumers, then it will do so, provided the macroeconomic effects are not too severe. In most cases it won’t even try to measure the extent of the cost-shifting; one will note, forexample, that the Commonwealth’s PBS statistics, while being extensive for subsidizedpharmaceuticals, are silent when it comes to non-subsidized prescriptions.
processes. Its concern has become a narrow financial focus on its own outlays – in this casePBS subsidies. If it can achieve budgetary savings through cost-shifting on to other parties,such as consumers, then it will do so, provided the macroeconomic effects are not too severe. In most cases it won’t even try to measure the extent of the cost-shifting; one will note, forexample, that the Commonwealth’s PBS statistics, while being extensive for subsidizedpharmaceuticals, are silent when it comes to non-subsidized prescriptions.