clinical case
CYSTINE CALCULI: MULTIDISCIPLINARY CHALLENGE Elaine Bronzatto, Daniel Silva Division of Urology - UNICAMP
CLINICAL BACKGROUND Eighteen year-old male is under treatment for recurrent stone disease since 10 years of age. He underwent several surgical interventions including percutaneous nephrolithotomy on left side, open pielolithotomy on left side and repeated extracorporeal shockwave lithotripsy (ESWL) session bilaterally.
CLINICAL WORKUP Laboratorial : cystinuria, hypomagnesuria and hypophosphaturia
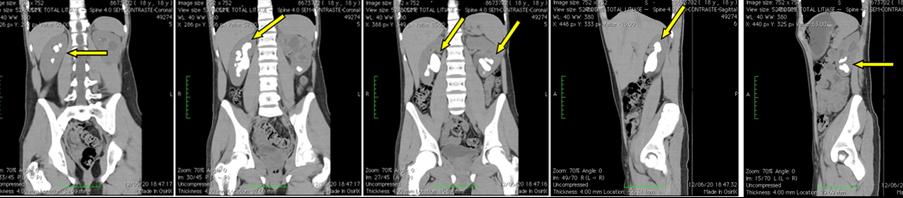
Figure 1 – Non contrast abdominal CT scan, coronal and sagital cuts, showing a grade II staghorn calculi on right side and multiple calculi in inferior calyx on left side (arrows).
MANAGEMENT Right percutaneous nephrolithotomy was performed (figure 2)
Figure 2 – Percutaneous nephrolithotomy. A) Patient in ventral position with marking (left posterior axilary line, 12th rib edge). B) Access to collecting system and placement of guidewire down the ureter. C) Final aspect: residual fragments and double J catheter.
FOLLOW UP Patient was kept under hypossodic diet, with red meat restriction and fluid intake over 2 liters/day. Potassium citrate 2g/ day; magnesium oxide 100mg/ day; pyridoxine 40 mg/day; captopryl 50 mg/day.
------------------------------------------------------------------------------------------------
O tratamento desse paciente é um desafio – calculo coraliforme bilateral (parcial no lado esquerdo). Estou de acordo com a indicação de nefrolitotripsia percutânea. Eu gostaria de puncionar o cálice superior, risco um pouco maior mas com melhor resultado em cálculos grandes, especialmente em associado com nefroscopio flexível (1). A punção é feita em expiração forçada, utilizando orientação endoscópica para ter uma punção acurada de onde introduzir a agulha (2). Nesse ponto os cálculos residuais no rim direito podem ser tratados com ureteroscopia flexível. O calculo do lado esquerdo, seria melhora acesso percutâneo através do cálice superior. Eu prefiro o cálice superior em todos os casos com configuração ramificada porque possibilita maior acesso com nefroscopio rígido para tratamento de cálculos grandes com litotridor ultrassônico. O paciente deverá fazer avaliação quantitativa de cistina em urina de 24 horas,
devendo ser considerado tratamento com Thiola (alfa-mercatopropionil-glicina).
References: 1. Wong C, Leveillee RJ. J Endourol. 2002 Sep;16(7):477-81. 2. Isac W, Rizkala E, Liu X, Noble M, Monga M. Urology. 2013 Feb;81(2):251-6. doi: 10.1016/j.urology.2012.10.004.
------------------------------------------------------------------------------------------------
Lillian Moneiro Pereira Clinica do Rim e Hipertensão de Campinas
Cystinuria is an inherited autosomal recessive disease in which cystine transportation through renal proximal tubules is deficient which in turn leads to urinary over saturation. Cystine calculi occur in 1 to 2% of patients with stone disease (and can reach 5% in pediatric population). It must be suspected whenever stone is formed in early infant age or teenage and when staghorn calculi is diagnosed. Lack of adequate response to extracorporeal shockwave lithotripsy may also rise suspicion of cystine calculi since these are extremely resistant (although less opaque than calcium oxalate stones).
Diagnosis is based upon calculi chemical analysis or through visualization of hexagonal crystals which are known to be pathognomonic in urinalysis (up to 25% of cases), especially when family history is positive.
In the absence of identifiable calculi or crystals, work up begins with a qualitative urinalysis of cystine (reference value:negative) – positive value indicates a urinary concentration of at least 75 mg/ml. Whenever one finds a positive result, a quantitative analysis is mandatory in a 24 hours urine colection specimen. A normal value should be lower than 50 mg/1,73m2/day. In cystinuria cases, excretion is usually higher than 400 mg/1,73m2/day. In the present case, urine excretion was 1485 mg/day and pharmacological treatment was affected.
The basis of treatment relies on keeping a cystine urinary concentration lower than solubility level, which is 243 mg/L on average under a pH higher than 7. As such, in the current case a minimal urinary volume of 6 liters would be necessary to avoid supersaturation and crystal formation. Besides, this volume would be needed throughout daytime and night time. Maintanance of such
high urine volume is not achievable and therefore complementary pharmacological therapy was needed.
Sodium diet restriction (<100 mEq/day): diminishes cystine excretion Protein diet restriction (0,8–1 g/kg/day): diminishes cystine production Urine alkalinization: enhances cystine solubility in a pH higher than 7 or 7,5; we preferentially usepotassium citrate (upto 3 to 4 mEq/kg/day in 4 separate intakes). Sodium bicarbonate should be avoided as a sodium overload nmay occur leading to higher cystine excretion (except for hyperkalemia cases). In selected cases, acetazolamide may be associated. Metabolic acidosis, however, must be monitored. Drugs containing thiol: contain sulphydryl groups that reduce disulphide bonds to protein molecules which composes cystine crystals enhancing their solubility. Main examples in this category are:
D-penicilamine: high severe side effects rate including aplastic anemia Tiopronin: fair results in some clinical cases, but similar poor safety profile as D-penicilamina
Captopryl: disulphide bonds captopryl-cystein are more soluble than cystine; however, the recommended therapeutic dose may reach 150 mg/day, leading to intolerable hypotensive side effect. Dose must be titrated to a maximum clinically acceptable level.
Periodical monitoring of cystine daily excretion is recommended. Although several pharmacological agents are available for clinical treatment of cystinuria, many patients maintain calculi formation and demand multiple surgical interventions.
Multiple interventions and repeated inefficient ESWL sessions may explain the progressive decrease in renal function in many of these patients, although kidney transplant is rarely needed. If this is the case, however, disease does not recur since the graft normally performs cystine transportation.
Still in experimental phase, the ester dimetil L-cystine inhibits crystal formation and may be an important addition to the therapeutic armamentarium against this devastating disease.
Palacin, M, Goodyer, P et al. Cystinuria. In: The Metabolic and Molecular Basis of Inherited Disease, 8th Ed, Scriver, CR, Beaudet, AL, Sly, WS, Valle, D (Eds), McGraw-Hill, New York 2001. p.4909
Mattoo A, Goldfarb DS. Cystinuria. Semin Nephrol 2008; 28:181.
Tiselius HG. New horizons in the management of patients with cystinuria. Curr Opin Urol 2010; 20:169.
Copelovitch L. Urolithiasis in children. Pediatr Clin North Am 2012 Aug; 59 (4): 881-96
Giving blood for your own use is a decision unused units. If the autologous units are not that will be made by you and your physician. used by the patient, the units will be discarded The term for this process is autologous donation. The following information is Why can I donate for myself more often than designed to help you make the decision that I can as a regular donor? G
The CAM in UME Project http://www.caminume.ca This material is made available through The CAM in UME Digital Resource Repository and is owned and copyrighted by the credited author(s). Materials are provided for educational purposes only. All copied materials must contain clear and proper citation. CAM IN UME AT DALHOUSIE 2006: CAM BASICS URL: http://www.cami

 clinical case
clinical case 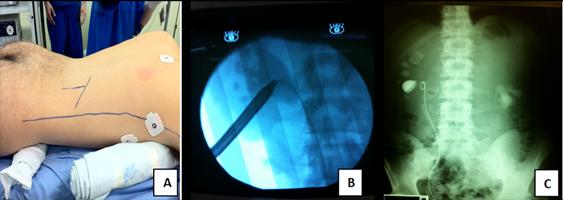 Figure 2 – Percutaneous nephrolithotomy. A) Patient in ventral position with marking (left posterior axilary line, 12th rib edge). B) Access to collecting system and placement of guidewire down the ureter. C) Final aspect: residual fragments and double J catheter.
FOLLOW UP Patient was kept under hypossodic diet, with red meat restriction and fluid intake over 2 liters/day. Potassium citrate 2g/ day; magnesium oxide 100mg/ day; pyridoxine 40 mg/day; captopryl 50 mg/day.
------------------------------------------------------------------------------------------------
O tratamento desse paciente é um desafio – calculo coraliforme bilateral (parcial no lado esquerdo). Estou de acordo com a indicação de nefrolitotripsia percutânea. Eu gostaria de puncionar o cálice superior, risco um pouco maior mas com melhor resultado em cálculos grandes, especialmente em associado com nefroscopio flexível (1). A punção é feita em expiração forçada, utilizando orientação endoscópica para ter uma punção acurada de onde introduzir a agulha (2). Nesse ponto os cálculos residuais no rim direito podem ser tratados com ureteroscopia flexível. O calculo do lado esquerdo, seria melhora acesso percutâneo através do cálice superior. Eu prefiro o cálice superior em todos os casos com configuração ramificada porque possibilita maior acesso com nefroscopio rígido para tratamento de cálculos grandes com litotridor ultrassônico. O paciente deverá fazer avaliação quantitativa de cistina em urina de 24 horas,
devendo ser considerado tratamento com Thiola (alfa-mercatopropionil-glicina).
References:
Figure 2 – Percutaneous nephrolithotomy. A) Patient in ventral position with marking (left posterior axilary line, 12th rib edge). B) Access to collecting system and placement of guidewire down the ureter. C) Final aspect: residual fragments and double J catheter.
FOLLOW UP Patient was kept under hypossodic diet, with red meat restriction and fluid intake over 2 liters/day. Potassium citrate 2g/ day; magnesium oxide 100mg/ day; pyridoxine 40 mg/day; captopryl 50 mg/day.
------------------------------------------------------------------------------------------------
O tratamento desse paciente é um desafio – calculo coraliforme bilateral (parcial no lado esquerdo). Estou de acordo com a indicação de nefrolitotripsia percutânea. Eu gostaria de puncionar o cálice superior, risco um pouco maior mas com melhor resultado em cálculos grandes, especialmente em associado com nefroscopio flexível (1). A punção é feita em expiração forçada, utilizando orientação endoscópica para ter uma punção acurada de onde introduzir a agulha (2). Nesse ponto os cálculos residuais no rim direito podem ser tratados com ureteroscopia flexível. O calculo do lado esquerdo, seria melhora acesso percutâneo através do cálice superior. Eu prefiro o cálice superior em todos os casos com configuração ramificada porque possibilita maior acesso com nefroscopio rígido para tratamento de cálculos grandes com litotridor ultrassônico. O paciente deverá fazer avaliação quantitativa de cistina em urina de 24 horas,
devendo ser considerado tratamento com Thiola (alfa-mercatopropionil-glicina).
References: