Intrahepatic cholestasis of pregnancy: a randomized controlled trial comparing dexamethasone and ursodeoxycholic acid
Intrahepatic Cholestasis of Pregnancy: a Randomized
Controlled Trial Comparing Dexamethasone and
Anna Glantz,1 Hanns-Ulrich Marschall,2 Frank Lammert,3 Lars-Åke Mattsson1
Intrahepatic cholestasis of pregnancy (ICP) is characterized by troublesome maternal pru- ritus, elevated serum bile acids (>10 mol/L) and increased fetal risk. Recently we deter- mined a cutoff level of serum bile acids, >40 mol/L, to be associated with impaired fetal outcome. We have now studied the effects of ursodeoxycholic acid (UDCA) and dexameth- asone on pruritus, biochemical markers of cholestasis, and fetal complication rates in a double-blind, placebo-controlled trial. For this purpose, 130 women with ICP were ran- domly allocated to UDCA (1 g/day for three weeks), or dexamethasone (12 mg/day for 1 week and placebo during weeks 2 and 3), or placebo for 3 weeks. Pruritus and biochemical markers of cholestasis were analyzed at inclusion and after 3 weeks of treatment. Fetal complications (spontaneous preterm delivery; asphyxial events; and meconium staining of amniotic fluid, placenta, and membranes) were registered at delivery. An intention-to-treat analysis showed significant reduction of alanine aminotransferase (ALT) (P ؍ .01) and bilirubin (P ؍ .002) in the UDCA group only. In a subgroup analysis of ICP women with serum bile acids >40 mol/L at inclusion (n ؍ 34), UDCA had significant effects on pruritus (؊75%), bile acids (؊79%), ALT (؊80%), and bilirubin (؊50%) as well, but not on fetal complication rates. Dexamethasone yielded no alleviation of pruritus or reduction of ALT and was less effective than UDCA at reducing bile acids and bilirubin. In conclusion, 3 weeks of UDCA treatment improved some biochemical markers of ICP irrespective of disease severity, whereas significant relief from pruritus and marked reduction of serum bile acids were only found in patients with severe ICP. (HEPATOLOGY 2005;42:1399-1405.)
Intrahepatic cholestasis of pregnancy (ICP) is a tion.1 Although essentially benign from a maternal
liver disease of as yet undefined etiology and
viewpoint, ICP is associated with increased fetal risks,
pathogenesis. ICP is characterized by pruritus and
such as preterm delivery in 19% to 60%,2-4 fetal distress in
elevated serum bile acids (Ն10 mol/L) with onset in the
22%-41%,3,5-8 and intrauterine fetal death in 1% to 4%
second half of pregnancy and persisting until delivery.
of affected pregnancies.3,6,9 Fetal complication rates are
Family clustering and varying incidence in different geo-
related to maternal serum bile acid levels, and increase
graphic regions suggest an underlying genetic explana-
when bile acid levels exceed 40 mol/L.10 Previous stud-ies have indicated that it is possible to reduce pruritus andsome surrogate parameters of cholestasis by pharmaco-
Abbreviations: ICP, intrahepatic cholestasis of pregnancy; UDCA, ursodeoxy-
logic treatment. Agents such as phenobarbital, anion ex-
cholic acid; ALT, alanine aminotransferase; ALP, alkaline phosphatase; ITT, in-
changers, S-adenosyl methionine, and others have been
From the Department of Obstetrics and Gynecology, Sahlgrenska University
tested but not introduced into clinical practice due to
Hospital/East, Go¨teborg, Sweden; Department of Medicine, Karolinska University
uncertain efficacy and/or intolerable side effects.11-13
Hospital Huddinge, Stockholm, Sweden; and Department of Internal Medicine I,University Hospital Bonn, Bonn, Germany.
However, small studies with ursodeoxycholic acid
Received July 26, 2005; accepted September 19, 2005.
(UDCA) and dexamethasone indicate that pharmaco-
Supported by grants from FoU, Va¨stra Go¨taland.
logic treatment may provide relief from pruritus and re-
Address reprint requests to: Anna Glantz, M.D., Department of Obstetrics andGynecology, Sahlgrenska University Hospital/East, 416 85 Go¨teborg, Sweden. E-
duce serum bile acid and liver enzyme levels. UDCA has
mail: [email protected]; fax: (46) 31 25 43 87.
been tested in two randomized, placebo-controlled stud-
Copyright 2005 by the American Association for the Study of Liver Diseases.
ies, with 8 patients in each group.14,15 The effects of dexa-
Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/hep.20952
methasone were investigated in an uncontrolled study of
Potential conflict of interest: Nothing to report.
10 women.16 These studies were not able to prove the
effectiveness of any of these treatments. Thus, we per-
capsules to be filled with dexamethasone, all of identical
formed a randomized, placebo-controlled trial aiming at
appearance, were supplied by Dr. Falk Pharma (Freiburg,
comparing the effects of UDCA and dexamethasone on:
Germany). The hospital pharmacy at Sahlgrenska Uni-
(i) alleviation of pruritus, (ii) improvement in serum liver
versity Hospital, Go¨teborg, filled the empty capsules with
tests, and (iii) the possible reduction of fetal complication
dexamethasone, packed study drugs in anonymous tins
rates after a treatment period of 3 weeks in women with
marked with a study code, and was responsible for ran-
domization. The study drugs were randomized in blocksof 6 treatments, containing 2 each of UDCA, dexameth-
Patients and Methods
asone, and placebo. Staff at the 6 participating centers
Between February 1, 1999, and January 31, 2002, all
were instructed to hand out the treatments consecutively,
pregnant women in the Va¨stra Go¨taland region of Swe-
starting with the lowest study code number. When all 6
den were prospectively screened for ICP, defined as oth-
treatments in the block were dispensed or when 6 months
erwise unexplained pruritus of pregnancy combined with
had elapsed, a new block was distributed.
fasting bile acid levels Ն10 mol/L. There were
The primary outcome variable was the rate of the fol-
1,500,462 inhabitants in the region in February 2001,
lowing fetal complications, registered at delivery and
and 45,485 pregnancies leading to deliveries during the
compared between groups: spontaneous preterm delivery
study period. In Sweden, all pregnancies are monitored by
(Ͻ37 weeks) in singleton pregnancies, asphyxial events
midwives in local prenatal clinics. If complications occur,
(operative delivery due to asphyxia, postpartum pH
women are referred to the nearest department of obstet-
Ͻ7.05 in umbilical arterial blood or Apgar score Ͻ7 at 5
rics for further care. All 106 prenatal clinics and all 6
minutes), and meconium staining of amniotic fluid, pla-
departments of obstetrics in the region participated in the
centa, and membranes. Changes of biochemical markers
and pruritus were secondary variables for evaluation. Dif-
During the study period, 937 women (2.1%) com-
ferences between groups regarding other obstetric vari-
plained of generalized pruritus during pregnancy and
ables such as total prematurity rate (including preterm
were, after giving written consent, included in the obser-
inductions of labor and preterm Caesarean sections), total
vational part of the ICP study. A study protocol recording
elective delivery rate (inductions of labor and planned
data on heredity, prior pregnancies, skin disorders, aller-
Caesareans), and maternal blood loss during vaginal de-
gic conditions, and hepatic, biliary, and metabolic condi-
tions was given to each patient. Puncture of an antecubital
Blood samples were analyzed for bile acids, amin-
vein was performed after a 12-hour fast to determine se-
otransferases, and bilirubin at inclusion, after 2-3 days,
rum bile acids on a weekly basis until parturition. If serum
after 4-5 days and after 1, 2, and 3 weeks of treatment. If
bile acids exceeded 10 mol/L at any time, the woman
the pregnancy continued after completed treatment, the
was diagnosed with ICP and referred to the nearest de-
same variables were analyzed weekly until parturition.
partment of obstetrics for further care. ICP was detected
Treatment effects on biochemical markers of cholesta-
in 693 women (1.5%). The results of the observational
sis and pruritus were evaluated as the differences between
part of our ICP study have recently been published.10
values at inclusion and after 3 weeks of treatment. Total
Women with ICP and a gestational age less than 37
serum bile acid concentrations were analyzed with an en-
weeks were invited to participate in a double-blind, pla-
zymatic, colorimetric method (Enzabile, Biostat Diagnos-
cebo-controlled study comparing treatment effects of
tic Systems, Stockport, UK). Aminotransferases and
UDCA and dexamethasone. Exclusion criteria were dia-
serum bilirubin levels were analyzed with standard labo-
betes, pre-eclampsia, intrauterine growth restriction, liver
ratory methods. Pruritus was estimated on a 100-mm–
disease (including viral hepatitis), and history of manic
long visual analog scale with the endpoints “no pruritus at
disorders or bleeding gastric ulcer. After exclusion, 425
all” (0 mm) and “worst possible pruritus” (100 mm).
Fetal well-being was monitored by cardiotocography at
Women who chose to participate were consecutively
enrolled after giving written consent. In a double-blind
The results of the serum analyses were open to the
fashion, they were randomly allocated to 1 of 3 groups.
managing obstetricians, who were not given any specific
The first group received UDCA, 1 g/day as a single dose,
instructions regarding timing of deliveries. The study was
for 3 weeks. The second group was allocated to dexameth-
approved by the Swedish Medical Products Agency and
asone, 12 mg/day as a single dose for 1 week, and placebo
the Ethics Committee of the Faculty of Medicine at the
during weeks 2 and 3. The third group was given placebo
University of Go¨teborg. All enrolled women gave written
for 3 weeks. UDCA capsules, placebo capsules, and empty
informed consent, according to the Helsinki declaration. Table 1. Obstetric and Biochemical Characteristics at Inclusion Dexamethasone Variable All included n ؍ 130 UDCA n ؍ 47 Placebo n ؍ 47 P Value
NOTE. Onset of pruritus, maternal and gestational age at inclusion, and biochemical variables are expressed as means Ϯ SD. Intensities of pruritus are expressed
Statistical Analysis.
and bilirubin at inclusion did not differ between groups,
medians, and ranges were calculated for descriptive pur-
nor did median values of pruritus intensity (Table 1).
The majority of the women (96 of 130) had bile acid
The Wilcoxon signed rank test was used for ordinal
levels of 10-39 mol/L at inclusion. A severe form of ICP
variables and for tests over time within groups. Changes
with bile acid levels Ն40 mol/L was identified in 34
over time between all 3 groups were analyzed by the
women (12 women in the UDCA group and in 11
Kruskal-Wallis test, and the Mann-Whitney U test was
women in the dexamethasone and placebo groups, respec-
used for pairwise comparisons. Comparisons of patient
characteristics and fetal and maternal outcome were
Treatment Effects on Maternal and Fetal Compli-
tested with the chi-square test or StudentЈs t test, as ap-
cation Rates. Fetal and maternal complication rates are
propriate. P values less than .05 were considered statisti-
presented in Table 2. The results are presented as inten-
tion-to-treat (ITT) analysis (Table 2A) and as a subgroup
Our estimation of the number of patients needed to
analysis in women with severe ICP (Table 2B). Sponta-
treat to observe differences in fetal complication rates be-
neous preterm deliveries in singleton pregnancies and to-
tween the UDCA, dexamethasone, and placebo groups
tal prematurity rate and meconium staining of amniotic
was based on fetal complication rates previously reported
fluid, placenta, and membranes were approximately dou-
in the literature.2-9 Based on a possible drug-related re-
bled in the severe ICP group, whereas the rates of asphyx-
duction of the fetal complication rate by 33%, a signifi-
ial events and total elective delivery did not differ when
cance level of 0.05, a two-tailed analysis, and a power of
these parameters in the ITT group were compared with
80%, 240 patients (80 in each arm) were needed to treat.
those of women with severe ICP. Treatment with UDCA
A subgroup analysis of changes in laboratory parame-
or dexamethasone did not improve any outcome variable
ters and pruritus during treatment was performed in ICP
in the ITT analysis group or in the subgroup of women
women with serum bile acids Ն40 mol/L at inclusion.
This analysis was based on the data from our recent ob-
Treatment Effects on Biochemical Markers and
servational study10 in which complication rates did not
Pruritus. Changes in bile acids, ALT, bilirubin, and
increase until serum bile acid values exceeded 40 mol/L.
pruritus during treatment with UDCA, dexamethasone,and placebo are presented in Fig. 1 as an ITT analysis
including all women (filled lines) and as a subanalysis of
A total of 130 women met the inclusion criteria and
women with bile acid levels Ն40 mol/L at inclusion
chose to participate in the treatment study. A total of 47
were randomized to UDCA, 36 to dexamethasone, and
ITT analysis (n ϭ 130) revealed significant reductions
47 to placebo. There were no differences between groups
in ALT (Fig 1B, P ϭ .01) and bilirubin (Fig. 1C, P ϭ
regarding parity or previous history of ICP. Mean values
.002) in the UDCA group compared with the placebo
(ϮSD) of pruritus onset; maternal and gestational age;
group. Changes in bile acids and pruritus did not reach
and levels of bile acids, alanine aminotransferase (ALT),
statistical significance. Overall, no significant changes
Table 2A. Fetal Complication Rates and Outcomes of Pregnancies: ITT Analysis All Included Dexamethasone UDCA n ؍ 47 Placebo n ؍ 47 P Value
were revealed during treatment with dexamethasone or
pruritus scores paralleled bile acid levels. Median pruritus
score on a visual analog scale was 74 mm at inclusion,
In women presenting with severe ICP (Ն40 mol/L)
increasing to 79 mm after 2-3 days of treatment. There
at inclusion (n ϭ 34), serum bile acid levels were reduced
was a subsequent decrease to 72 mm after 4-5 days of
by treatment both in the UDCA (Ϫ79%) and in the
treatment and further to 55, 27, and 18 mm after 1, 2,
dexamethasone (Ϫ45%) groups, compared with placebo
and 3 weeks of treatment, respectively.
(ϩ13%) (P ϭ .001 and P ϭ .01, respectively). The re-
Tolerability and Duration of Treatment. The du-
duction was more pronounced in the UDCA group than
ration of treatment is illustrated in Table 3. A total of 80
in the dexamethasone group (P ϭ .001; Fig. 1A). In the
women completed the 3-week treatment period. One
UDCA group, serum bile acid levels increased from
woman in each group discontinued because of side effects
101 Ϯ 58 mol/L to 153 Ϯ 111 mol/L during the first
within 3 days (UDCA, 1 patient after 3 days because of
2-3 days of treatment. After 4-5 days the values decreased
diarrhea; dexamethasone, 1 patient after 2 days because of
to 115 Ϯ 105 mol/L, and further to 83 Ϯ 77; 36 Ϯ 52;
nausea, dizziness, and stomach pain; placebo, 1 patient
and 21 Ϯ 13 mol/L after 1, 2, and 3 weeks of treatment,
after 1 day because of severe headache). One woman in
respectively. The initial decrease of bile acids in the dexa-
each group was randomized to treatment but did not start
methasone group was rapid but transient, from 71 Ϯ 22
medication because of fear of side effects. The remaining
to 26 Ϯ 26 mol/L after the first week of treatment, but
women discontinued their treatment because of sponta-
rising again to 39 Ϯ 22 mol/L after 3 weeks of treat-
Adverse Events. One case of intrauterine fetal death
A reduction in ALT was only found in the UDCA
occurred during the study period. The subject was a 26-
group (UDCA vs. dexamethasone: P ϭ .002, UDCA vs.
year-old woman undergoing her first pregnancy, who was
placebo: P ϭ .01, Fig. 1B). A reduction in bilirubin was
medicated with clomipramine, 10 mg daily, due to a long-
observed both in the UDCA group and in the dexameth-
term depressive disorder with anxiety and panic attacks.
asone groups vs. placebo (P Ͻ .001 and P ϭ .001, respec-
Her pruritus started in week 33, and she was allocated to
tively; Fig. 1C). Pruritus was alleviated only in the UDCA
treatment in week 36. Bile acid levels were 16 mol/L
group and differed significantly from the dexamethasone
both at inclusion and after 2 weeks of treatment. cardio-
group (P ϭ .01) and the placebo group at the end of
tocography was normal at check-up visits after 1 and 2
treatment (P ϭ .001; Fig. 1D). In the UDCA group,
weeks of treatment. Two days after her last check-up,
Table 2B. Fetal Complication Rates and Outcomes of Pregnancies: Subanalysis of ICP Women With Bile Acids >40 mol/L Dexamethasone All n ؍ 34 (%) UDCA n ؍ 12 (%) n ؍ 11 (%) Placebo n ؍ 11 (%) P Value
NOTE. Fetal complication rates and outcomes of pregnancies as an ITT analysis (A), and a subgroup analysis in women with bile acid levels Ն40 mol/L at inclusion
*Spontaneous onset of labor Ͼ37 weeks in singleton pregnancies. †Operative delivery due to asphyxia, arterial umbilical pH Ͼ7.05, or Apgar Score Ͻ7 at 5 minutes of age. ‡Including multiple pregnancies and iatrogenous prematurity. §The sum of planned deliveries, including inductions of labor and caesarean sections.
Fig. 1. Mean levels of serum bile acids (A), ALT (B), bilirubin (C), and median of pruritus scores (D) in women with ICP at inclusion and after 3
weeks of treatment with ursodeoxycholic acid (UDCA), dexamethasone (dexa) and placebo. Filled lines represent results in the ITT group (n ϭ 130)and dotted lines show results in the subgroup analysis of women with severe ICP (Ն40 mol/L) at inclusion. (A) Serum bile acids mol/L; means). No changes were observed after ITT analysis. In women with severe ICP at inclusion, both UDCA and dexamethasone reduced bile acids, comparedto placebo (UDCA vs. placebo: P ϭ .001, dexamethasone vs. placebo: P ϭ .01). UDCA was more effective than dexamethasone (UDCA vs. dexamethasone: P ϭ .001). (B)Serum ALT (U/L; means). ITT analysis showed a reduction of ALT in the UDCA group vs. placebo (P ϭ .01). In womenwith severe ICP at inclusion, ALT was reduced only in the UDCA group (UDCA vs. dexamethasone: P ϭ .002; UDCA vs. placebo: P ϭ .01;dexamethasone vs. placebo: n.s.). (C) Serum bilirubin (mol/L; means). ITT showed a reduction of bilirubin in the UDCA group vs. placebo (P ϭ.002). In women with severe ICP at inclusion, bilirubin was reduced both in the UDCA and dexamethasone group vs. placebo (P Ͻ .001 and P ϭ.001, respectively), but UDCA was proven to be more effective than dexamethasone within the group over time (UDCA: P Ͻ .001, dexamethasone:P ϭ .04). (D) Pruritus score (visual analog scale, 0 mmϭno pruritus, 100 mmϭworst possible pruritus; medians). No changes were observed afterintent-to-treat analysis. In women with severe ICP at inclusion, UDCA was more effective than dexametasone (P ϭ .01) and placebo (P ϭ .001),and a reduction of pruritus within the group over time was only noticed in the UDCA group (UDCA: P ϭ .001; dexamethasone: n.s.; placebo: n.s.).
spontaneous labor began. Intrauterine fetal death was di-
was unable to demonstrate differences between treatment
agnosed in the delivery ward, and the patient delivered a
groups regarding fetal complication rates. According to
stillborn baby (birth weight, 3650 g). The amniotic fluid
power calculations based on previously published fetal
was heavily meconium stained. No autopsy was per-
complication rates in women with ICP, 240 women
formed. The incident was reported to the Swedish Med-
should have been included, 80 in each arm. Only 130 of
ical Products Agency as an adverse event. When the study
425 eligible women, according to inclusion criteria, ac-
code was broken, it was revealed that this woman had
cepted participation. The most common explanation for
not entering the study was fear of negative treatment ef-fects on the fetus, which may be the major obstacle to
Discussion
clinical studies of pharmacologic agents in pregnant
Intrahepatic cholestasis of pregnancy has been re-
women, presumably not only in Sweden. It is noteworthy
ported to be associated with maternal pruritus and in-
that even if 240 women had been included, it would have
creased fetal risk, including intrauterine fetal death.2-9
been insufficient to reveal treatment effects on fetal out-
This double-blind, placebo-controlled study was de-
come because the overall number of fetal complications
signed to compare the effects of UDCA and dexametha-
was substantially lower in our ICP study population than
sone on fetal outcome, biochemical markers of
cholestasis, and maternal pruritus in women diagnosed
However, because the observational part of our ICP
with ICP. Based on an ITT analysis, the only observed
study recently demonstrated that fetal complication rates
significant effects of any treatment were UDCA-induced
do not increase until bile acid levels exceed 40 mol/L,10
reductions of serum bilirubin and ALT levels. The study
the subgroup of women presenting with bile acid levels
Ն40 mol/L at randomization was analyzed separately. This subgroup analysis revealed that treatment with
Table 3. Duration of Treatment
UDCA actually improved all biochemical markers of cho-
Dexamethasone
lestasis as well as pruritus, and that treatment with UDCA
P Value
was more effective than treatment with dexamethasone or
placebo. Mean bile acid levels decreased by 79% in the
UDCA group, compared with a 45% decrease in the
dexamethasone group and a 13% increase in the placebogroup (UDCA vs. dexamethasone, P
Duration of therapy in 3 groups of women with ICP, randomized to treatment
with ursodeoxycholic acid (UDCA), dexamethasone, or placebo for 3 weeks.
placebo, P ϭ .001). In this subgroup analysis, the UDCA-
induced reductions of ALT (by 80%) and bilirubin (by
study medication was strictly double blind, and the ran-
50%) were more pronounced than in the ITT analysis
domization procedure was performed by a professional
and also differed significantly from the ALT and bilirubin
authority. However, boxes containing the study medica-
reductions observed in the dexamethasone (ALT, Ϫ17%;
tion had to be replaced at the study centers every 6
bilirubin, Ϫ22%) and placebo groups (ALT, Ϫ18%; bil-
months, regardless of whether all study medications had
irubin, Ϫ11%; for ALT, UDCA vs. dexamethasone: P ϭ
been used or not. Some study centers did not include
.002; UDCA vs, placebo: P ϭ .01). However, although
more than 1 or 2 patients durinig every 6-month period
the relative incidence of a number of fetal complications
of, leading to a large amount of study medication not
such as preterm delivery, meconium passage and green-
being used, which might have had an impact on the dif-
staining of placenta/membranes was approximately twice
as high in women with bile acids exceeding 40 mol/L
In this study, both UDCA and dexamethasone were
compared with women with bile acid levels Ͻ40 mol/L
well tolerated, with similar discontinuation rates. The rea-
(Table 2), the subanalysis did not reveal any difference in
son for choosing only 1 week of active treatment followed
the outcome related to treatment with UDCA or dexa-
by 2 weeks of placebo in the dexamethasone group was
that this is the only dose regimen of dexamethasone treat-
The efficacy of UDCA in ICP pregnancies has been
ment in ICP pregnancies previously reported in the liter-
previously investigated in 2 small randomized, placebo-
ature.16 Furthermore, questions have recently been raised
controlled ICP trials, both with 8 patients in the UDCA
concerning potentially harmful effects of corticosteroids
group and treatment periods of 20 days. One study
on the developing fetal brain. This has lead to a more
showed a reduction of all investigated variables (pruritus,
restrictive approach to corticosteroid treatment during
bile acids, bilirubin, and alkaline phosphatase [ALP]) in
pregnancy,17,18 The data from the present study showed
the UDCA group, but also a significant reduction in pru-
that dexamethasone was less effective than UDCA regard-
ritus and ALP in the placebo group.14 The other study
ing all studied variables. Therefore we conclude that
showed a decrease of aminotransferases, bilirubin, and
UDCA is currently the best pharmacologic treatment op-
pruritus in the UDCA group, but no reduction of bile
acids,15 which is in line with the results of our study.
Proof of the efficacy of UDCA, in particular the effect
Efficacy in reducing maternal serum bile acid levels seems
on fetal complication rates, nevertheless remains to be
to be an important quality when choosing a drug for the
elicited from investigations of an even larger study popu-
treatment of ICP because bile acid levels have been dem-
lation. We propose a serum bile acid level of Ն40 mol/L
onstrated to have a dose-dependent association with fetal
as the lower limit for inclusion of patients.
complication rates.10 In conflict with a previous report on
In conclusion, ITT analysis showed that UDCA reduced
dexamethasone therapy in ICP women,16 we found the
ALT and bilirubin, but not bile acids or pruritus, in women
effects on pruritus and biochemical markers of cholestasis
with ICP. In patients with bile acid levels exceeding 40
to be transient in the dexamethasone group. A rapid de-
mol/L, treatment with UDCA was more effective in alle-
crease in pruritus and bile acids was seen after the first
viating pruritus and reducing bile acids, aminotransferases,
week of treatment, but was followed by an increase.
and bilirubin, compared with treatment with dexametha-
An interesting detail was the observation of an increase
sone and placebo. However, no differences in fetal or mater-
of total serum bile acid levels during the first 2-3 days of
nal complication rates could be detected. Although this is as
treatment in the UDCA group, decreasing close to base-
yet the largest treatment study of ICP, the sample size was
line after 4-5 days of treatment, after which a steady de-
still too small to answer the important question of whether
crease occurred. This phenomenon was interpreted as a
fetal complications in ICP can be reduced by pharmacologic
dose-dependent medication effect, initially adding supra-
treatment. Nevertheless, our data may help to define inclu-
physiological levels of UDCA to the total maternal bile
sion criteria for an even larger, multicenter, double-blind,
acid pool. Interestingly, the pruritus scores paralleled the
placebo-controlled study of UDCA for the treatment of ICP
serum bile acid levels, increasing in the first days of treat-
ment and then gradually decreasing. Thus, from a clinicalviewpoint, the efficacy of UDCA treatment in bile acid
level reduction in ICP cannot be evaluated earlier than
wives in the Va¨stra Go¨taland region for enrolling and
taking care of study patients. Study nurse Ann Christians-
The fact that the randomized groups differed in size
son was of invaluable help. Special thanks to Anders Ode´n
(dexamethasone n ϭ 36, UDCA and placebo n ϭ 47,
and Emma Jaensson for their help with the statistical cal-
respectively) is surprising. The random allocation to the
References
11. Heikkinen J, Maentausta O, Ylo¨stalo P, Janne O. Serum bile acid levels in
intrahepatic cholestasis of pregnancy during treatment with phenobarbital
1. Lammert F, Marschall HU, Glantz A, Matern S. Intrahepatic cholestasis of
or cholestyramine. Eur J Obstet Reprod Biol 1982;14:153-162.
pregnancys: molecular pathogenesis, diagnosis and management. J Hepa-
12. Ribalta J, Reyes H, Gonzalez MC, Iglesias J, Arrese M, Poniachik J, et al.
S-Adenosyl-L-methionine in the treatment of patients with intrahepatic
2. Reid R, Ivey KJ, Rencoret RH, Storey B. Fetal complications of obstetric
cholestasis of pregnancy: a randomized, double-blind placebo controlled
study with negative results. HEPATOLOGY 1991;18:1084-1089.
3. Fisk NM, Storey GN. Fetal outcome in obstetric cholestasis. Br J Obstet
13. Roncaglia N, Locatelli A, Arreghini A, Assi F, Cameroni I, Pezzullo J, et al.
A randomised controlled trial of ursodeoxycholic acid and S-adenosyl-l-
4. Rioseco AJ, Ivankovic MB, Manzur A, Hamed F, Kato SR, Parer JT, et al.
methionine in the treatment of gestational cholestasis. BJOG 2004;111:
Intrahepatic cholestasis of pregnancy: a retrospecive case-control study of
14. Diaferia A, Nicastri PL, Tartagni M, Loizzi P, Iacovizzi C, Di Leo A.
perinatal outcome. Am J Obstet Gynecol 1994;170:890-895.
Ursodeoxycholic acid therapy in pregnant women with cholestasis. Int J
5. Shaw D, Frolich J, Wittman BA, Willms M. A prospective study of 18
patients with cholestasis of pregnancy. Am J Gynecol 1982;142:621-625.
15. Palma J, Reyes H, Ribalta J, Hernandez I, Sandoval L, Almuna R, et al.
6. Laatikainen T, Ikonen E. Fetal prognosis in obstetric cholestasis. Ann Chir
Ursodeoxycholic acid in the treatment of cholestasis of pregnancy: a ran-
domized, double-blind study controlled with placebo. J Hepatol 1997;27:
7. Laatikainen T, Tulenheimo A. Maternal serum bile acid levels and fetal
distress in cholestasis of pregnancy. Int J Gynecol Obstet 1984;22:91-94.
16. Hirvioja ML, Tuimala R, Vuori J. The treatment of Intrahepatic cholesta-
8. Laatikainen T. Fetal bile acid levels in pregnancies complicated by mater-
sis of pregnancy by dexamethasone. Br J Obstet Gynaecol 1992;99:109-
nal intrahepatic cholestasis. Am J Obstet Gynecol 1975;122:852-856.
9. Alsulyman OM, Ouzounian JG, Ames-Castro M, Goodwin TM. Intrahe-
17. Abbasi S, Hirsch D, Davis J, Tolosa J, Stouffer N, Debbs R, et al. Effect on
patic cholestasis of pregnancy: perinatal outcome associated with expectant
single versus multiple courses of antenatal corticosteroids on maternal and
management. Am J Obstet Gynecol 1996;175:957-960.
neonatal outcome. Am J Obstet Gynecol 2000;182:1243-1249.
10. Glantz A, Marschall HU, Mattsson LA. Intrahepatic cholestasis of preg-
18. Thorp JA, Jones PG, Knox E, Clark RH. Does antenatal corticosteroid
nancy. Relationships between bile acid levels and fetal complication rates.
therapy affect birth weight and head circumference? Obstet Gynecol 2002;
Eva Nilsson a,), Henrik von Euler b, Jaak Berendson a, Anders Thorne cIngemar Naslund d, Anne-Sofie Lagerstedt b, Kristina Narfstrom b, Jerker M. Olsson ea Department of Chemical Engineering and Technology, Applied Electrochemistry, Royal Institute of Technology ( b Department of Small Animal Clinical Sciences, Swedish Uni Õ ersity of Agricultural Sciences ( c Department of Surgery, Hu
Production 2013 Rules/Regulations and Suggestions • Please be on time! We have a limited time in the High School and lots to accomplish. • Attendance for all three nights (black rehearsal, dress rehearsal and the production) is mandatory. • No costume is to be worn to the rehearsal. Dressing rooms will be assigned for you to change. • Please keep the costum
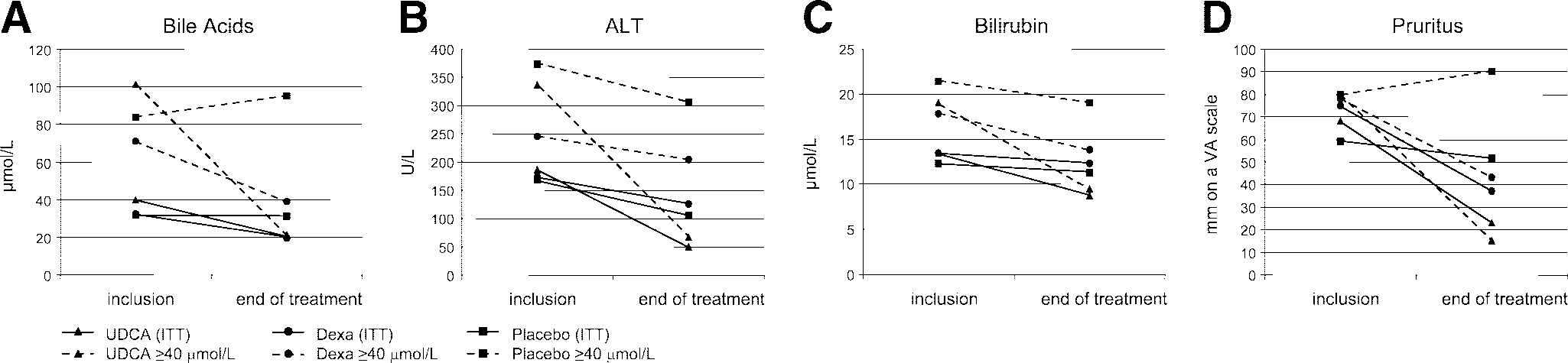 Fig. 1. Mean levels of serum bile acids (A), ALT (B), bilirubin (C), and median of pruritus scores (D) in women with ICP at inclusion and after 3
weeks of treatment with ursodeoxycholic acid (UDCA), dexamethasone (dexa) and placebo. Filled lines represent results in the ITT group (n ϭ 130)and dotted lines show results in the subgroup analysis of women with severe ICP (Ն40 mol/L) at inclusion. (A) Serum bile acids mol/L; means).
Fig. 1. Mean levels of serum bile acids (A), ALT (B), bilirubin (C), and median of pruritus scores (D) in women with ICP at inclusion and after 3
weeks of treatment with ursodeoxycholic acid (UDCA), dexamethasone (dexa) and placebo. Filled lines represent results in the ITT group (n ϭ 130)and dotted lines show results in the subgroup analysis of women with severe ICP (Ն40 mol/L) at inclusion. (A) Serum bile acids mol/L; means).