Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Ohr.tulane.edu
R e v i e w s / C o m m e n t a r i e s / A D A S t a t e m e n t s Hypoglycemia, Diabetes, and Cardiovascular Events YRUS V. DESOUZA, MD EREMIA B. BOLLI, MD
leading to an increase in severe hypogly-
IVIAN FONSECA, MD
cemia with brain dysfunction (9,11). Theresponse of adrenaline (and norepineph-rine) in individuals with hypoglycemia
Diabetesisatepidemicproportions Whilethereasonfortheincreasedmor- unawarenessislowerthaninawaresub-
tality is unclear and hypoglycemia has not
jects (9), a finding that might be of car-
been implicated as a cause of death, these
of glycemic control in decreasing the risk
the degree of glycemic control required to
quite varied in the literature (supplemen-
tary Table 1, available in an online appen-
complications has been controversial.
with lack of standardization of definition
Several large clinical trials looking at this
DEFINITION, INCIDENCE
of hypoglycemia and its classification.
issue have either shown no benefit or even
OF, AND RISK FACTORS ASSOCIATED WITH
trials reviewed in this article depends on
glycemia as a risk factor for cardiovascular
HYPOGLYCEMIA — The modern
the definitions of mild, moderate, and se-
events is a topic of much debate. In this
definition of hypoglycemia is plasma glu-
vere hypoglycemia. Most recent large tri-
review article, we discuss the evidence for
cose Ͻ70 mg/dl (7–9). At plasma glucose
below this threshold (60 – 65 mg/dl), the
sible mechanisms that might be involved.
motes secretion of counterregulatory hor-
those that are self-treated (supplementary
creased risk of cardiovascular disease.
nized as a major barrier to achieving nor-
firmly established (1,2). However, the as-
“rapid” responses), which have relevant
cardiovascular effects (9 –11). This occurs
has therefore been investigated in terms of
its impact (particularly on cognitive func-
tion) and physiological counterregulation
sive glucose control has often failed to re-
at lower plasma glucose (Ͻ60 mg/dl) (9).
glucose control invariably increases the risk
cur often over time (e.g., once a day), the
ity of hypoglycemia (2) Several epidemio-
creased cardiovascular risk (3–5). Recent
higher levels (i.e., it takes a lower plasma
large randomized trials looking at inten-
glucose to activate symptom responses) is
group treated with insulin (1). In the 4-T
no benefit (Action in Diabetes and Vascu-
glucose decreases to Յ50 mg/dl. In turn,
patient per year were lowest in the basal
insulin group (1.7), higher in the biphasic
mia in an early phase (hypoglycemia
aspart insulin group (3.0), and highest in
unawareness) increases the risk of pro-
cular Risk in Diabetes [ACCORD]) (6).
tients reported that the duration of diabe-tes and the duration of insulin treatment
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1University of Nebraska Medical Center, Omaha, Nebraska; the 2Section of Internal Medicine and
glycemic episodes (15). Thus, although in
Oncology, University of Perugia, Italy; and the 3Tulane University Health Sciences Center, New Orleans,Louisiana.
general in type 2 diabetes there is less hy-
Corresponding author: Cyrus Desouza, [email protected].
Received 11 November 2009 and accepted 9 March 2010.
with increased diabetes and insulin treat-
2010 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.
org/licenses/by-nc-nd/3.0/ for details.
DIABETES CARE, VOLUME 33, NUMBER 6, JUNE 2010
Hypoglycemia and cardiovascular events
(8), primarily because of loss of glucagon
the forefront the question of the role of
risk for cardiovascular events. There are
after artificial ventilation. Nineteen others
aged Ն65 years, who used insulin or sul-
few studies looking at this question.
were sleeping alone at the time of death,
Broadly, they can be divided into studies
that look at the effect of hypoglycemia on
(23). Gill et al. (24) demonstrated that, in
(16). In this cohort, recent hospital dis-
patients with type 1 diabetes, severe hy-
charge was the strongest predictor of sub-
MYOCARDIAL ISCHEMIA, INFARCTION, AND
tive study of 267 patients with both type 1
ARRHYTHMIAS — The earliest
study in 1932 reported chest pain consis-
glycemic events in 155 patients (17). Pa-
CEREBRAL ISCHEMIA,
seven type 1 diabetic patients with known
STROKE, AND DEMENTIA — Severe hypoglycemia
these findings (3,5). More recently, in a
with coronary artery disease, recruited for
correction of blood glucose. However, the
with type 2 diabetes. Predictors of diabe-
tes in this group included previous hypo-
glycemia and duration of insulin therapy.
A retrospective cross-sectional analysis in
to assess the efficacy of bezafibrate in re-
dysfunction and dementia. Whitmer et al.
symptoms in 12% of diet-treated patients,
Israel) over an 8-year mean follow-up, hy-
study of 16,667 patients with type 2 dia-
30% of patients on insulin (18). Risk fac-
betes looking at the relationship between
hazard ratio of 1.84, but not of increased
coronary artery disease mortality (4). The
found that the attributable risk of demen-
after institution of intensive glycemic con-
trol versus standard control (32 vs. 20%)
cognitive dysfunction has been associated
(20). However, this was not significantly
risk of severe hypoglycemia (hazard ratio
2.1) in patients with type 2 diabetes (26).
Diabetes (BARI 2D) trial, although severe
glycemia itself was not found to increase
major cardiovascular events were not sig-
the risk of getting dementia (27). In type 1
cise, alcohol, older age, renal dysfunction,
infection, decreased intake of energy, and
ations in regional cerebral blood flow in
mental health issues, including dementia,
depression, and psychiatric illnesses. In
EPIDEMIOLOGICAL EVIDENCE FOR THE ASSOCIATION BETWEEN
cemia. Less studied is the “dead-in-bed”
blood flow in patients with type 1 diabe-
HYPOGLYCEMIA AND CARDIOVASCULAR
nocturnal death in type 1 diabetes. In one
these are temporary and reversible (28). It
MORBIDITY — Recent studies such
is unclear whether this finding can be ex-
DIABETES CARE, VOLUME 33, NUMBER 6, JUNE 2010
Desouza, Bolli, and Fonseca
intensive insulin protocols to control in-
risk for dementia is still controversial.
increased risk of hypoglycemia in the in-
tensive treatment arm, there was no asso-
from these trials have increased the con-
ROLE OF HYPOGLYCEMIA
troversy over the risks versus benefit of
IN THE RESULTS OF RECENT
cardiovascular mortality (30). One expla-
tight inpatient glycemic control. Van den
CLINICAL TRIALS — Recently, sev-
eral large randomized trials evaluating the
tensive insulin therapy in critically ill pa-
effects of glycemic control on cardiovas-
tients reduced morbidity and mortality.
cular events have published their results
farction) study found that insulin-glucose
10,251 participants with a history of car-
infusion followed by intensive subcutane-
diovascular events or significant cardio-
ous insulin in diabetic patients with acute
trial had a 2- to 3-year shorter duration of
halted because of a significant increase in
ority of insulin versus conventional treat-
study. The relative risk of death associ-
account for the low level of hypoglycemia
cose Insulin in Stroke Trial (GIST)-U.K.
looked at tight control of glucose in pa-
for the intensive arm versus 2.87 for the
tients with acute stroke using an intensive
standard arm in spite of larger number of
rolled type 1 diabetic patients on insulin
tensive arm. This suggests that severe hy-
treatment. In contrast to the UK Diabetes
poglycemia in a certain subset of patients
than the strategy of treatment used (inten-
tional” treatment group (0.19 episodes/
data are based on post hoc analysis, and the
tality rate of 34 versus 22% for those who
true cause of the increased mortality in these
risk in the “intensive” group (0.62 epi-
subset of patients most prone to the detri-
mental effects of hypoglycemia had several
of the following characteristics: they were
increased cardiovascular mortality (13) at
likely to be women, African American, older
later follow-up (1). This indirectly high-
patients, or patients with a longer duration
lights the different cardiovascular risk of
volume and insulin therapy in severe sep-
hypoglycemia in type 2 versus type 1 dia-
betes. Thus, it is clear that these trials had
different treatment strategies to achieve risk
with type 2 diabetes to an intensive treat-
study by Kosiborod et al. (40), looking at
appreciate that the strategy used to achieve
group (31). At the end of the study, there
risk factor modification is important in how
dial infarction, found that a J-shaped re-
was no significant difference in cardiovas-
it affects patient outcomes. Moreover, the
particular strategy’s effect on a risk factor
arms. As expected, there was an increased
may not predict its effect on patient out-
incidence of severe hypoglycemia in the in-
tensive treatment group. Predictors for hy-
poglycemia included increased duration of
HYPOGLYCEMIA AND
diabetes, insulin treatment at baseline, low
INPATIENT GLUCOSE
steeper in patients with diabetes, suggest-
CONTROL — Hyperglycemia is com-
mon in acutely ill patients and is associ-
creased mortality, especially in diabetic
patients. In another study, a pooled anal-
11,140 participants to an intensive glyce-
mortality (33). This has subsequently led
to a large number of trials using various
DIABETES CARE, VOLUME 33, NUMBER 6, JUNE 2010
Hypoglycemia and cardiovascular events
ies, death occurred in 4.6% of the patientswith hypoglycemia versus 1% of thosewho were considered euglycemic (81–199 mg/dl) (41). In contrast, a sub-analysis of the DIGAMI 2 data did notshow hypoglycemia to be an independentrisk factor for future morbidity or mortal-ity in patients with type 2 diabetes andmyocardial infarction (42).
diovascular mortality in the inpatient set-ting is still controversial. Much of thevariability in results is due to the differentprotocols used, differences in definitionof hypoglycemia, as well as methodologyof its detection and report, presence orabsence of safeguards against hypoglyce-mia in the protocols, local training level ofthe personnel administering the proto-cols, and selected patient population. Hence, carefully constructed clinical trailsto research this question are required. However, it is prudent to conclude fromthe available data that severe hypoglyce-mia should be avoided as much as possi-
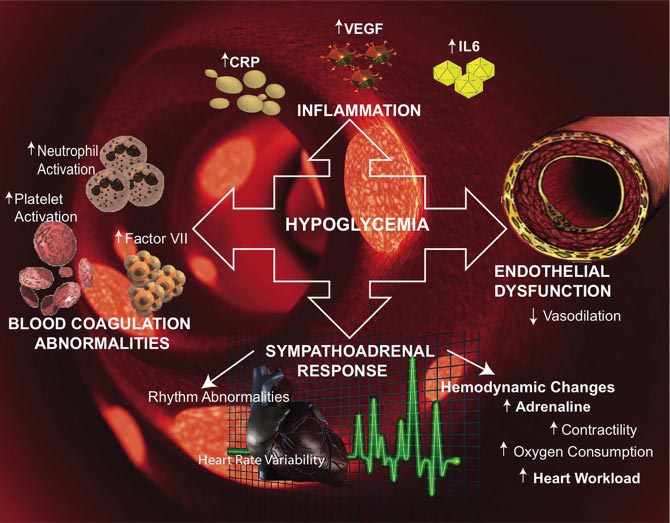
Figure 1—Mechanisms by which hypoglycemia may affect cardiovascular events. Hypoglycemicevents may trigger inflammation by inducing the release of C-reactive protein (CRP), IL-6, andvascular endothelial growth factor (VEGF). Hypoglycemia also induces increased platelet andneutrophil activation. The sympathoadrenal response during hypoglycemia increases adrenalineMECHANISMS BY WHICH secretion and may induce arrhythmias and increase cardiac workload. Underlying endothelialdysfunction leading to decreased vasodilation may also contribute to cardiovascular risk.HYPOGLYCEMIA MAY AFFECT CARDIOVASCULAR EVENTS — Hypoglycemia induces
rate variability have been associated with
several counterregulatory responses.
-cell insulin secretion, an increase in glycemia is associated with a significant ies did not find any associations betweenpancreatic ␣-cell glucagon secretion, an
heart rate variability, hypoglycemia, and
(QTC) in subjects with and without diabetes
increased catecholamine release (10,46).
(10,24). Other electrocardiographic abnor-
and norepinephrine (in addition to its ele-
malities observed during hypoglycemia in-
INFLAMMATION,
vated tissue turnover), as well as an in-
COAGULATION, AND
creased secretion of ACTH/glucocorticoids.
moderate ST segment depressions (10). ENDOTHELIAL
Besides these classical responses, there are
DYSFUNCTION DURING
several indirect changes induced by hypo-
HYPOGLYCEMIA — Inflammation
glycemia that affect inflammatory cytokine
secretion, endothelial function, coagula-
in particular could lead to a high risk of
tion, and fibrinolysis. All of these responses
have potential adverse effects on cardiovas-
cular morbidity and mortality and will be
vented or reversed by  blockade (43). THE SYMPATHOADRENAL
result in endothelial injury and abnormal-
RESPONSE — Hypoglycemia stimu-
cardiac repolarization abnormalities.
ities in coagulation, resulting in increased
lates the release of catecholamines, which
These effects can be reversed by  block-
risk for cardiovascular events (Fig. 1).
Certain growth factor levels such as vas-
and blood vessels. Catecholamines increase
myocardial contractility, myocardial work-
increased locally and in circulation after
ulation may contribute to the occurrence of
disease (3). The greater oxygen demand is
adverse cardiac events (44). Abnormalities
of hypoglycemia, thus perpetuating a pos-
not met because of the rigid vessels, but also
in high-frequency and low-frequency heart
DIABETES CARE, VOLUME 33, NUMBER 6, JUNE 2010
Desouza, Bolli, and Fonseca
tis, Novo Nordisk, Takeda, Pfizer, sanofi-
glycemia in healthy subjects. Ann Noninva-
in platelet function and activation of the
aventis, Eli Lilly, and the American Diabetes
Association. He has also received honoraria for
11. Sherwin RS. Bringing light to the dark side
epinephrine levels lead to an increase in
of insulin: a journey across the blood-brain
Kline, Novartis, Novo Nordisk, Takeda, Pfizer,
sanofi-aventis, Eli Lilly, and Daiichi Sankyo.
12. Cryer PE: Hypoglycemia in Diabetes: Patho-physiology, Prevalence and Prevention. Alex-
of these changes can be reversed by ␣ or 
Nordisk and Takeda for consulting. No other
andria, VA, American Diabetes Association,
potential conflicts of interest relevant to this
13. Hypoglycemia in the Diabetes Control and
Complications Trial. The Diabetes Control
acute hypoglycemia. Vessel wall stiffness
and Complications Trial Research Group. References
glycemia in patients with type 1 diabetes
1. Gore MO, McGuire DK. The 10-year post-
14. Holman RR, Farmer AJ, Davies MJ, Levy
JC, Darbyshire JL, Keenan JF, Paul SK, 4-T
Study Group. Three-year efficacy of com-plex insulin regimens in type 2 diabetes.
diovascular observations in context. Diab
cardiovascular events, especially in a sub-
15. UK Hypoglycaemia Study Group. Risk of
set of patients with longer duration of di-
abetes. As discussed before, this has been
effects of treatment modalities and their du-
suggested as a possible explanation for the
3. Egeli ES, Berkmen R. Action of hypogly-
ration. Diabetologia 2007;50:1140 –1147
16. Shorr RI, Ray WA, Daugherty JR, Griffin
MR. Incidence and risk factors for serious
dysfunction are closely interdependent.
17. Donnelly LA, Morris AD, Frier BM, Ellis JD,
aggravating factors that contribute to in-
marker for increased long-term mortalityrisk in patients with coronary artery dis-
G, Leese GP, DARTS/MEMO Collaboration.
cardiovascular disease, longer duration of
5. Judson WE, Hollander W. The effects of
diabetes: a population-based study. Diabet
thy (Fig. 1). However, most of these stud-
with angina pectoris: before and after in-
18. Miller CD, Phillips LS, Ziemer DC, Gallina
ies are short-duration acute observations
and the long-term effects of hypoglycemia
in patients with type 2 diabetes mellitus.
6. Skyler JS, Bergenstal R, Bonow RO, Buse J,
19. Strouse SSS, Katz LN, Rubinfield SH.
Treatment of older diabetic patients with
man MS, Kosiborod M, Reaven P, Sher-win RS, American Diabetes Association,
CONCLUSIONS — The review of the
20. Abraira C, Colwell J, Nuttall F, Sawin CT,
literature and results from large random-
ized trials suggest that severe hypoglyce-
of cardiovascular events: implications of
NV, Levin SR, Pacold I, Lee HS. Cardiovas-
cular events and correlates in the Veterans
in type 1 and type 2 diabetes. This is true
Affairs Diabetes Feasibility Trial. Veterans
in the outpatient setting as well as the in-
entific Statement of the American College
Control and Complications in Type II Dia-
patient setting. Although smaller observa-
betes. Arch Intern Med 1997;157:181–188
ican Heart Association. J Am Coll Cardiol
21. BARI 2D Study Group, Frye RL, August P,
cemia and cardiovascular events, there is
7. American Diabetes Association. Standards
currently no evidence for causality. Larger
of medical care in diabetes—2010. Diabetes
clinical trials looking specifically at this
question are required. The mechanisms that
8. Cryer PE. Hypoglycemia: still the limiting
Sobel BE. A randomized trial of therapies for
type 2 diabetes and coronary artery disease.
9. Rossetti P, Porcellati F, Bolli GB, Fanelli
22. Desouza C, Salazar H, Cheong B, Murgo J,
patients is to lower blood glucose to near-
normal values to lower the risk for long-
1 diabetes: the role of insulin analogs.
mia-associated morbidity and mortality.
10. Laitinen T, Lyyra-Laitinen T, Huopio H,
deaths of type 1 diabetic patients. Diabet
Vauhkonen I, Halonen T, Hartikainen J, Ni-
Acknowledgments — V.F. has received re-
24. Gill GV, Woodward A, Casson IF, Weston
search support from GlaxoSmithKline, Novar-
alterations during hyperinsulinemic hypo-
DIABETES CARE, VOLUME 33, NUMBER 6, JUNE 2010
Hypoglycemia and cardiovascular events
poglycaemia in type 1 diabetes: the ‘dead
42. Mellbin LG, Malmberg K, Waldenstro¨m
in bed’ syndrome revisited. Diabetologia
34. Van den Berghe G, Wilmer A, Hermans G,
25. Whitmer RA, Karter AJ, Yaffe K, Quesen-
glycaemic episodes during hospitalisation
for myocardial infarction in patients with
R. Intensive insulin therapy in the medical
type 2 diabetes: a report from the DIGAMI
patients with type 2 diabetes mellitus.
43. Robinson RT, Harris ND, Ireland RH, Lee
study of intensive insulin treatment on long
term survival after acute myocardial infarc-
tion in patients with diabetes mellitus.
cia G, Neal B, Pan CY, Patel A, Poulter N,
cose Infusion in Acute Myocardial Infarc-
44. Adler GK, Bonyhay I, Failing H, Waring E,
36. Malmberg K, Ryde´n L, Wedel H, Birkeland
function: implications for rigorous glycemic
Fisher M, Hamsten A, Herlitz J, Hildebrandt
45. Vlcek M, Radikova Z, Penesova A, Kvet-
nansky R, Imrich R. Heart rate variability
Waldenstro¨m A, DIGAMI 2 Investigators.
Intense metabolic control by means of insu-
27. Bruce DG, Davis WA, Casey GP, Clarnette
lin in patients with diabetes mellitus and
acute myocardial infarction (DIGAMI 2): ef-
Huikuri HV, Perkio¨ma¨ki JS. Effects of
37. NICE-SUGAR Study Investigators, Finfer S,
Chittock DR, Su SY, Blair D, Foster D, Dh-
polarisation in patients with type 1 diabe-
ingra V, Bellomo R, Cook D, Dodek P, Hen-
derson WR, He´bert PC, Heritier S, Heyland
Frier BM. Regional cerebral blood flow in
IDDM patients: effects of diabetes and of
mia induces a rise in C-reactive protein.
BG, Ronco JJ. Intensive versus conventional
glucose control in critically ill patients.
48. Razavi Nematollahi L, Kitabchi AE, Kitab-
29. Action to Control Cardiovascular Risk in
O’Connell JE, Johnston DE, Cartlidge NE,
Trialists Collaboration. Glucose-potassi-
JL, Simons-Morton DG, Friedewald WT.
mic stress in healthy subjects. Metabolism
49. Dantz D, Bewersdorf J, Fruehwald-Schul-
30. ADVANCE Collaborative Group, Patel A,
39. Brunkhorst FM, Engel C, Bloos F, Meier-
HL, Peters A. Vascular endothelial growth
MacMahon S, Chalmers J, Neal B, Billot L,
saint R, Welte T, Schaefer M, Kern P, Ku-
50. Del Rey A, Roggero E, Randolf A, Mahuad
C, McCann S, Rettori V, Besedovsky HO.
Bompoint S, de Galan BE, Joshi R, Travert F.
IL-1 resets glucose homeostasis at central
levels. Proc Natl Acad Sci U S A 2006;103:
51. Dalsgaard-Nielsen J, Madsbad S, Hilsted
J. Changes in platelet function, blood co-
31. Duckworth W, Abraira C, Moritz T, Reda
agulation and fibrinolysis during insulin-
FA, Marso SP, Spertus JA. Glucometrics in
dial infarction: defining the optimal out-
52. Fisher BM, Hepburn DA, Smith JG, Frier
complications in veterans with type 2 di-
41. Pinto DS, Skolnick AH, Kirtane AJ, Mur-
32. Krumholz HM, Lee TH. Redefining qual-
ity: implications of recent clinical trials.
53. Sommerfield AJ, Wilkinson IB, Webb DJ,
33. Capes SE, Hunt D, Malmberg K, Gerstein
Frier BM. Vessel wall stiffness in type 1 dia-
betes and the central hemodynamic effects
risk of death after myocardial infarction in
tion myocardial infarction. J Am Coll Car-
of acute hypoglycemia. Am J Physiol Endo-
patients with and without diabetes: a sys-
DIABETES CARE, VOLUME 33, NUMBER 6, JUNE 2010
Szemle DEMOKRÁCIA Az emberi egyenértékûség Krisztus- sal kezdõdik, ezért nincs és nem is lehet felebaráti de-mokrácia Krisztus és tanítása nélkül. (1974. július 1.)Ha a kisebbség erõlteti rá akaratát a többségre, eznem demokrácia, hanem egészen másvalami. (1948. Az igazi demokrácia alappillére, hogy sértetlen O R S Z Á G G Y Û L É S természetj
Slutrapport Revision av dokumentation, klassificering och registrering av vårdkontakter inom öppenvård vid Nacka Närsjukhus Proxima AB 25 maj 2011 Staffan Bryngelsson Emendor Consulting AB Innehållsförteckning: Två besök samma datum 2009 och 2010 . 4 6.3 DRG 970O Sjuksköterskebesök 2010 . 10 6.4 Revisorernas sammanfattade kommentarer . 11 7.
 Hypoglycemia and cardiovascular events
Hypoglycemia and cardiovascular events