Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Oandplibrary.net
Fungal colonisation in digital silicone rubber prostheses
M. E. L. LEOW*, A. K. KOUR*'****, T. J. J. INGLIS**'***,
G. KUMARASINGHE*** and R. W. H. PHO*'****
*Department of Orthopaedic Surgery, The National University of Singapore, Singapore **Department of Microbiology, The National University of Singapore, Singapore ***Department of Laboratory Medicine, National University Hospital, Singapore ****Department of Hand and Reconstructive Microsurgery, National University Hospital, Singapore Abstract
is recommended. Prior cleaning to remove
The fungal discolouration of silicone rubber
organic matter before decontamination is
prostheses is reported in four cases. In two of
the cases, the discolouration was caused by the fungus Candida tropicalis. In the other two
Introduction
cases, two different fungal organisms, namely
Silicone elastomers are widely used in the
Trichoderma sp. and Scedosporium prolificans
were incriminated. The non-porous silicone
prostheses. One of the problems identified with
rubber layers create an enclosed environment in
the use of this material is a black discolouration
the suction cup of the prosthesis and preclude
caused by fungal growth (Masella et al., 1975;
ventilation at the prosthesis-stump interface.
Makila and Hopsu-Havu, 1976; Pigno et ah,
The moisture as a result of sweat and body
1994). In nasal prostheses, this has been
warmth in the stump assists fungal growth.
attributed to the continual exposure to moist air
Residual salts from the sweat, sebum from
and secretions that constantly pass through the
nasal aperture. Although silicone digital
petroleum jelly (Vaseline™) applied to
prostheses have been prescribed to patients for
facilitate donning, can adhere to the surfaces of
over a decade (Pillet, 1983; Beasley, 1987;
the prosthesis and provide the nutrients for
Alison and McKinnon, 1992; Campbell et al.,
fungal growth. Prolonged continuous usages of
1992; Leow et al., 1996; Pereira et al, 1996;
the prosthesis, the presence of sweaty palms in
O'Farrell et al., 1996) there have been no
the users, donning me prosthesis during manual
reported incidences of fungal colonisation.
physical activities which induce perspiration,
However, the conditions associated with the use
washing of hands with the prosthesis on and
warm humid climatic conditions have been
identified as factors predisposing the prosthesis
to fungal colonisation. The fungal growth
discolouration in finger prostheses for which a
caused a black discolouration and marred the
aesthetic quality of the prostheses. As a preventative measure, daily immersion of the
Materials and methods
The authors have developed a custom-made
benzalkonium chloride, or water at 60°C for 15
digital prosthesis using a silicone elastomer
minutes, or decontamination with 70% alcohol
(Leow et al., 1996; Pereira et al., 1996). The prostheses are made from a medical grade of silicone elastomer (Cosmedica Ltd, Newport,
UK). Colour pigments (Cosmedica Ltd,
Professor Robert W. H. Pho, Department of
Newport, UK) are intrinsically mixed with the
Orthopaedic Surgery, The National University of
silicone to match the basic colour of the
Singapore, 10 Kent Ridge Crescent, Singapore
119260. Tel: (+65)7724340; Fax: (+65)7732558
patient's skin. No anti-fungal agents are
incorporated. The prostheses are moulded with layers of the silicone rubber tinted to differing
shades of colour, the outer layers of the
prostheses which correspond with the epidermis and superficial dermis are rendered translucent
while the inner layers which correspond to the inner dermis and subcutaneous tissues are
rendered opaque. This is to mimic the stratified
anatomy of the skin and achieve a life-like
Fig 2. Another prosthesis in which the black
appearance. A layer of touch-up colouration is
discolouration had invaded the translucent outer layers,
"sandwiched" between the layers of silicone
rubber at the finger joints and nail to enhance the details and colouration at these areas. The
with the black discolouration for examination
hollow part of the prosthesis which corresponds
under the light microscope using the xlO and
with the deficit in the segment is packed with a
filler material comprising a mixture of silicone
examined from end to end, with particular
elastomer and polystyrene beads. The contact
attention to the distribution of the black
surface of the silicone polystyrene core which
sits snugly on the distal stump is sealed with a layer of silicone rubber to prevent moisture
Laboratory investigations revealed fungal
In a follow-up review of 34 cases fitted with
the prostheses for over two years or more, four
discolouration. Brightfield microscopy showed
cases of black discolouration in the prostheses
a distinct layer of mycelial growth in the
caused by fungal growth were encountered
sections taken through the areas affected with
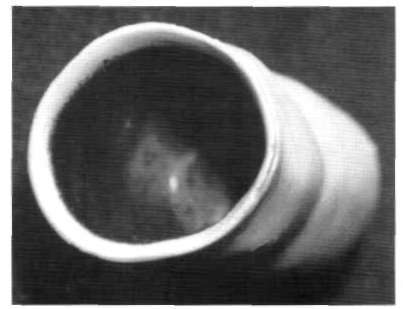
(Figs. 1 and 2). The discolouration was rough in
texture (Fig. 1) and found to be extremely
Laboratory investigations and microscopy:
resistant to cleaning with 70% alcohol. Besides
Various strains of bacteria were identified in the
the black discolouration, the problems of wear
scrapings from the affected areas of the
and tear and a yellowing discolouration caused
prostheses. These included Straphylococcus, Micrococcus, Corynebacterium spp., and
Laboratory investigations and microscopy: Flavobacterium meningosepticum. Three fungal
Scrapings were taken from the areas affected by
species were isolated from all the affected
the black discolouration for bacteriological and
prostheses, namely Candida tropicalis, from
myocological investigations. Transverse two of the cases, and Trichoderma sp. and sections were made through the areas affected
Scedosporium prolificans each from the other two cases. Investigations also reveal an invasion of the inner layers of the prostheses by fungal growth. Fungal hyphae were seen forming a distinct layer in the silicone material (Fig. 3).
The fungal discolouration was seen as black
spots and patches on the inner surfaces of the prosthesis in contact with the stump, including the sealed surfaces of the silicone-polystyrene core. In all four cases, the patients reported it to have occurred between 10-18 months post-fitting. This progressed to cover a wider area and
penetrated deeper into the material over a 3-4 week period with continued use (between 8-10 hours per day). As the outer layers of the prosthesis are translucent, the black
Fig 1. An affected prosthesis showing a black
discolouration became visible when the fungus
discolouration caused by fungal growth on the internal
penetrated through the opaque inner layers and
the silicone rubber prostheses affected with a similar discolouration. The non-porous property of silicone rubber added to the conditions associated with the use of the prostheses provided the conditions of moisture, warmth and nutritional support for fungal growth.
Entrapped perspiration in the suction cup prosthesis: A secure prosthetic fit created an
airtight seal between the non-porous prosthesis and the stump. Doffing of the prosthesis is achieved by creating an inlet for the entry of air to diffuse the vacuum effect. This same
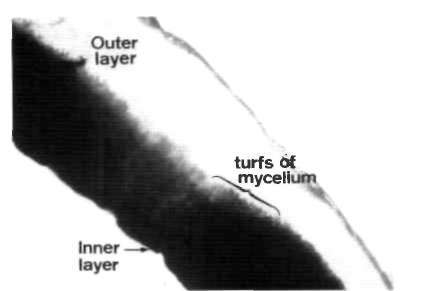
Fig 3. A transverse section through the affected areas of
requirement for a suction cup prosthetic fit has
the prosthesis (shown in Fig. 2) as seen under Brightfield
the disadvantage of precluding cutaneous
ventilation. It not only precipitates perspiration but traps the sweat on the stump when the
invaded the outer-inner layer interface. In one
prosthesis is donned for extended hours. The
case, the black discolouration had spread to the
problem can be compounded by a humid tropical
outer layers of the prosthesis causing an
climate. The moisture from perspiration and
body warmth of the stump provide an ideal
microscopic observation revealed turfs of fungal
hyphae (mycelia) invading the outer layers of
observation noted in these cases was the presence
the prosthesis (Fig. 3). The discolouration
of a sweaty palm. This is a contributing factor in
marred the aesthetic quality of the prosthesis.
promoting the conditions for fungal growth.
moist upon removal of the prosthesis. All
nutritional support is needed to sustain fungal
patients indicated perspiration in their stump as
growth. These nutrients can possibly come both
one of the problems they encountered with the
extrinsically and intrinsically from the inside
daily use of their prosthesis. No physical signs
surface of the prosthesis. The authors have
of fungal growth were observed on the stump in
noted in this study that patches of residues
any of the affected cases. There were no allergic
reactions in the stump in any of the four cases.
(Vaseline™) applied to facilitate donning,
However, two patients experienced discomfort
residual salts from sweat and sebum from the
due to the surface roughness (Fig. 1) created by
sebaceous secretions adhered to the inside
the fungal colonisation within the suction cup.
surface of the prosthesis. This provided the initial extrinsic nutritional requirements for
Discussion
fungal growth to start with. It is also possible
Various commensals are present in the skin.
that the vaseline and sebaceous secretion are
absorbed into the silicone material. This may
distribution are transient and vary from time to
provide the intrinsic source of nutrients which
time. Their multiplication is contained under
encouraged the fungus to penetrate into the
normal use of the hand. However, if there is an
increase in the level of moisture and warmth
Of relevance was the patients' care of the
with availability of nutritional support, some
prostheses. Instructions on the care of the
fungal species may thrive. In the silicone soft
prosthesis as advised to the patients included
lining (Silastic 390) of dentures, two fungus
cleaning the inner surfaces of the prosthesis
strains, Candida albicans and Candida
daily using a cotton-bud soaked with a mild
tropicalis were reported to be responsible for
the black discolouration often encountered with
bacterial and fungal growth, the importance of
their use (Masella et ai, 1975). In this study,
keeping the surfaces of the prosthesis dry was
Candida tropicalis and two other fungal
species, namely, Trichoderma sp. and
Scedosporium prolificans were incriminated in
prescribing a silicone rubber prosthesis to
prevent fungal growth. Masella and coworkers
(1975) showed that daily immersion of the
ALISON A, MACKINNON SE (1992). Evaluation of digital
dental prostheses in benzalkonium chloride
prostheses. J Hand Surg 17A, 923-926.
(Zephiran, Winthrop Laboratories, New York),
BEASLEY RW (1987). Hand and finger prostheses.
or water at 60°C for 15 minutes was found to be
JHandSurg 12A, 144-147.
an effective measure to prevent the growth of
CAMPBELL GS, GOW D, HOOPER G (1992). Low cost
the Candida albicans and Candida tropicalis in
cosmetic hand prostheses. J Hand Surg 17B, 201-203.
silicone lining on dentures. Since the black
discolouration in the finger prostheses of the
LEOW EL, KOUR AK, PEREIRA BP, PHO RWH (1996).
Colour-matching in hand and finger prostheses: the
above patients was caused by fungal invasion, a
Asian perspective. Hand Surg (Asia Pacific) 1, 37-43.
similar preventive measure could be adopted. Cleaning the inner surfaces of the prosthesis is
MAKILA E, HOPSU-HAVU VK (1976). Mycotic growth
and soft denture lining materials. Acta Odont Scand
important to remove dirt and grease before
immersing in a disinfectant, or before applying 70% alcohol for decontamination. Pigno et ah,
MASELLA RP, DOLAN CT, LANEY WR (1975). The
prevention of the growth of Candida on silastic 390
(1994) also found that using an antifungal agent
soft liner for dentures. J Prosthet Dent 33, 250-257.
(Clotrimazole) incorporated into the silicone
O'FARRELL DA, MONTELLA BJ, BAHOR JL, LEVIN LS
rubber elastomer was effective in inhibiting the
(1996). Long-term follow-up of 50 Duke silicone
growth of fungus in vitro. However, the clinical
prosthetic fingers. J Hand Surg 21B, 696-700.
application and long term results were not
PEREIRA BP, KOUR AK, LEOW EL, PHO RWH (1996).
Benefits and use of a digital prostheses. J Hand Surg 21A, 222-228. Acknowledgements
PIGNO MA, GOLDSCHMIDT MC, LEMON JC (1994). The
efficacy of antifungal agents incorporated into a facial
prosthetic silicone elastomer. J Prosthet Dent 71, 295
financial support provided by the National
Science and Technology Board through two
PILLET J (1983). Esthetic hand prostheses. J Hand Surg
A Hyper-Interactive Teaching Technology Company H-ITT LLC. 420 Shearer Blvd. Cocoa, Florida 32922 Instructors Guide for Using SoftClick SoftClick is an easy-to-use browser-based application for educational assessment that allows students to send answers using virtually any device that is web-enabled, such as laptops, cell phones and PDAs. SoftClick works with standard web br

 incorporated. The prostheses are moulded with layers of the silicone rubber tinted to differing
shades of colour, the outer layers of the
prostheses which correspond with the epidermis and superficial dermis are rendered translucent
while the inner layers which correspond to the inner dermis and subcutaneous tissues are
rendered opaque. This is to mimic the stratified
anatomy of the skin and achieve a life-like
Fig 2. Another prosthesis in which the black
appearance. A layer of touch-up colouration is
discolouration had invaded the translucent outer layers,
"sandwiched" between the layers of silicone
rubber at the finger joints and nail to enhance the details and colouration at these areas. The
with the black discolouration for examination
hollow part of the prosthesis which corresponds
under the light microscope using the xlO and
with the deficit in the segment is packed with a
filler material comprising a mixture of silicone
examined from end to end, with particular
elastomer and polystyrene beads. The contact
attention to the distribution of the black
surface of the silicone polystyrene core which
sits snugly on the distal stump is sealed with a layer of silicone rubber to prevent moisture
Laboratory investigations revealed fungal
In a follow-up review of 34 cases fitted with
the prostheses for over two years or more, four
discolouration. Brightfield microscopy showed
cases of black discolouration in the prostheses
a distinct layer of mycelial growth in the
caused by fungal growth were encountered
sections taken through the areas affected with
(Figs. 1 and 2). The discolouration was rough in
texture (Fig. 1) and found to be extremely
Laboratory investigations and microscopy:
resistant to cleaning with 70% alcohol. Besides
Various strains of bacteria were identified in the
the black discolouration, the problems of wear
scrapings from the affected areas of the
and tear and a yellowing discolouration caused
prostheses. These included Straphylococcus,
Micrococcus, Corynebacterium spp., and
Laboratory investigations and microscopy:
Flavobacterium meningosepticum. Three fungal
Scrapings were taken from the areas affected by
species were isolated from all the affected
the black discolouration for bacteriological and
prostheses, namely Candida tropicalis, from
myocological investigations. Transverse two of the cases, and Trichoderma sp. and sections were made through the areas affected
Scedosporium prolificans each from the other two cases. Investigations also reveal an invasion of the inner layers of the prostheses by fungal growth. Fungal hyphae were seen forming a distinct layer in the silicone material (Fig. 3).
The fungal discolouration was seen as black
spots and patches on the inner surfaces of the prosthesis in contact with the stump, including the sealed surfaces of the silicone-polystyrene core. In all four cases, the patients reported it to have occurred between 10-18 months post-fitting. This progressed to cover a wider area and
penetrated deeper into the material over a 3-4 week period with continued use (between 8-10 hours per day). As the outer layers of the prosthesis are translucent, the black
Fig 1. An affected prosthesis showing a black
discolouration became visible when the fungus
discolouration caused by fungal growth on the internal
penetrated through the opaque inner layers and
incorporated. The prostheses are moulded with layers of the silicone rubber tinted to differing
shades of colour, the outer layers of the
prostheses which correspond with the epidermis and superficial dermis are rendered translucent
while the inner layers which correspond to the inner dermis and subcutaneous tissues are
rendered opaque. This is to mimic the stratified
anatomy of the skin and achieve a life-like
Fig 2. Another prosthesis in which the black
appearance. A layer of touch-up colouration is
discolouration had invaded the translucent outer layers,
"sandwiched" between the layers of silicone
rubber at the finger joints and nail to enhance the details and colouration at these areas. The
with the black discolouration for examination
hollow part of the prosthesis which corresponds
under the light microscope using the xlO and
with the deficit in the segment is packed with a
filler material comprising a mixture of silicone
examined from end to end, with particular
elastomer and polystyrene beads. The contact
attention to the distribution of the black
surface of the silicone polystyrene core which
sits snugly on the distal stump is sealed with a layer of silicone rubber to prevent moisture
Laboratory investigations revealed fungal
In a follow-up review of 34 cases fitted with
the prostheses for over two years or more, four
discolouration. Brightfield microscopy showed
cases of black discolouration in the prostheses
a distinct layer of mycelial growth in the
caused by fungal growth were encountered
sections taken through the areas affected with
(Figs. 1 and 2). The discolouration was rough in
texture (Fig. 1) and found to be extremely
Laboratory investigations and microscopy:
resistant to cleaning with 70% alcohol. Besides
Various strains of bacteria were identified in the
the black discolouration, the problems of wear
scrapings from the affected areas of the
and tear and a yellowing discolouration caused
prostheses. These included Straphylococcus,
Micrococcus, Corynebacterium spp., and
Laboratory investigations and microscopy:
Flavobacterium meningosepticum. Three fungal
Scrapings were taken from the areas affected by
species were isolated from all the affected
the black discolouration for bacteriological and
prostheses, namely Candida tropicalis, from
myocological investigations. Transverse two of the cases, and Trichoderma sp. and sections were made through the areas affected
Scedosporium prolificans each from the other two cases. Investigations also reveal an invasion of the inner layers of the prostheses by fungal growth. Fungal hyphae were seen forming a distinct layer in the silicone material (Fig. 3).
The fungal discolouration was seen as black
spots and patches on the inner surfaces of the prosthesis in contact with the stump, including the sealed surfaces of the silicone-polystyrene core. In all four cases, the patients reported it to have occurred between 10-18 months post-fitting. This progressed to cover a wider area and
penetrated deeper into the material over a 3-4 week period with continued use (between 8-10 hours per day). As the outer layers of the prosthesis are translucent, the black
Fig 1. An affected prosthesis showing a black
discolouration became visible when the fungus
discolouration caused by fungal growth on the internal
penetrated through the opaque inner layers and
 the silicone rubber prostheses affected with a similar discolouration. The non-porous property of silicone rubber added to the conditions associated with the use of the prostheses provided the conditions of moisture, warmth and nutritional support for fungal growth.
Entrapped perspiration in the suction cup
prosthesis: A secure prosthetic fit created an
airtight seal between the non-porous prosthesis and the stump. Doffing of the prosthesis is achieved by creating an inlet for the entry of air to diffuse the vacuum effect. This same
Fig 3. A transverse section through the affected areas of
requirement for a suction cup prosthetic fit has
the prosthesis (shown in Fig. 2) as seen under Brightfield
the disadvantage of precluding cutaneous
ventilation. It not only precipitates perspiration but traps the sweat on the stump when the
invaded the outer-inner layer interface. In one
prosthesis is donned for extended hours. The
case, the black discolouration had spread to the
problem can be compounded by a humid tropical
outer layers of the prosthesis causing an
climate. The moisture from perspiration and
body warmth of the stump provide an ideal
microscopic observation revealed turfs of fungal
hyphae (mycelia) invading the outer layers of
observation noted in these cases was the presence
the prosthesis (Fig. 3). The discolouration
of a sweaty palm. This is a contributing factor in
marred the aesthetic quality of the prosthesis.
promoting the conditions for fungal growth.
moist upon removal of the prosthesis. All
nutritional support is needed to sustain fungal
patients indicated perspiration in their stump as
growth. These nutrients can possibly come both
one of the problems they encountered with the
extrinsically and intrinsically from the inside
daily use of their prosthesis. No physical signs
surface of the prosthesis. The authors have
of fungal growth were observed on the stump in
noted in this study that patches of residues
any of the affected cases. There were no allergic
reactions in the stump in any of the four cases.
(Vaseline™) applied to facilitate donning,
However, two patients experienced discomfort
residual salts from sweat and sebum from the
due to the surface roughness (Fig. 1) created by
sebaceous secretions adhered to the inside
the fungal colonisation within the suction cup.
surface of the prosthesis. This provided the initial extrinsic nutritional requirements for
Discussion
the silicone rubber prostheses affected with a similar discolouration. The non-porous property of silicone rubber added to the conditions associated with the use of the prostheses provided the conditions of moisture, warmth and nutritional support for fungal growth.
Entrapped perspiration in the suction cup
prosthesis: A secure prosthetic fit created an
airtight seal between the non-porous prosthesis and the stump. Doffing of the prosthesis is achieved by creating an inlet for the entry of air to diffuse the vacuum effect. This same
Fig 3. A transverse section through the affected areas of
requirement for a suction cup prosthetic fit has
the prosthesis (shown in Fig. 2) as seen under Brightfield
the disadvantage of precluding cutaneous
ventilation. It not only precipitates perspiration but traps the sweat on the stump when the
invaded the outer-inner layer interface. In one
prosthesis is donned for extended hours. The
case, the black discolouration had spread to the
problem can be compounded by a humid tropical
outer layers of the prosthesis causing an
climate. The moisture from perspiration and
body warmth of the stump provide an ideal
microscopic observation revealed turfs of fungal
hyphae (mycelia) invading the outer layers of
observation noted in these cases was the presence
the prosthesis (Fig. 3). The discolouration
of a sweaty palm. This is a contributing factor in
marred the aesthetic quality of the prosthesis.
promoting the conditions for fungal growth.
moist upon removal of the prosthesis. All
nutritional support is needed to sustain fungal
patients indicated perspiration in their stump as
growth. These nutrients can possibly come both
one of the problems they encountered with the
extrinsically and intrinsically from the inside
daily use of their prosthesis. No physical signs
surface of the prosthesis. The authors have
of fungal growth were observed on the stump in
noted in this study that patches of residues
any of the affected cases. There were no allergic
reactions in the stump in any of the four cases.
(Vaseline™) applied to facilitate donning,
However, two patients experienced discomfort
residual salts from sweat and sebum from the
due to the surface roughness (Fig. 1) created by
sebaceous secretions adhered to the inside
the fungal colonisation within the suction cup.
surface of the prosthesis. This provided the initial extrinsic nutritional requirements for
Discussion