Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Circadian rhythm sleep disorders (crsd)
Sleep Medicine Reviews, Vol. 6, No. 1, pp 45–55, 2002
doi:10.1053/smrv.2001.0190, available online at http://www.idealibrary.com on
MEDICINE Yaron Dagan
Institute for Fatigue and Sleep Medicine, “Sheba” Medical Center, Affiliated to “Sackler” Medical School,Tel Aviv University, Israel
KEYWORDS
Circadian Rhythm Sleep Disorders (CRSD) are a group of sleep disorders
characterized by a malsynchronization between a person’s biological clock and the
environmental 24-h schedule. These disorders can lead to harmful psychological and
functional difficulties and are often misdiagnosed and incorrectly treated due to the
fact that doctors are unaware of their existence. In the following review we describethe characteristics of CRSD, their diagnosis, treatment as well as their relationship
to psychopathology, psychotropic drugs and head trauma.
2002 Published by Elsevier Science Ltd
INTRODUCTION WHAT ARE CRSD?
The inborn human sleep-wake schedule is longer
Twenty years ago Weitzman et al. [5] first described
than 24 h. It is synchronized to the external 24-h
30 of their insomnia patients (7%) as suffering from
day, and reacts to environmental zeitgebers (time
Delayed Sleep Phase Syndrome (DSPS). These
cues). The environmental zeitgeber – bright light –
patients had a tendency to fall asleep very late at
seems to play the crucial role in this process [1, 2].
night and to experience difficulty rising at a desired
The sleep-wake schedule is synchronized also with
time in the morning. They also found that when
other circadian cycles in the body: body tem-
these patients were allowed to sleep without ex-
perature, and the secretion of: melatonin, growth
ternal restrictions, they slept for a normal lengthof time and exhibited no pathology in their sleep
architecture. Their patients were younger than
Human beings sleep at night and are awake during
other types of insomniacs, without differences of
the day. This essential phenomenon so taken for
sex prevalence, displaying no specific psychiatric
granted can become chronically impaired in some
disorders, and of various ages of onset. This dis-
people leading to a group of disorders called: Cir-
covery led to the recognition of the existence of
cadian Rhythm Sleep Disorders (CRSD) [3, 4].
Circadian Rhythm Sleep Disorders (CRSD) other
These disorders are usually unfamiliar to the phys-
ician thus frequently misdiagnosed and incorrectly
Today, the criteria for the definition and diagnosis
treated. The aim of this review is to shed light on
of CRSD (formerly Sleep Wake Schedule Disorders
these disorders: characteristics, diagnosis, treat-
– SWSD ) are described by the International
Classification of Sleep Disorders (ICSD) [3, 4]. According to this definition, CRSD constitute amisalignment between the patient’s sleep patternand that, which is desired or regarded as the societalnorm. Sleep episodes occur at inappropriate times
Correspondence should be addressed to: Y. Dagan, Institutefor Fatigue and Sleep Medicine, “Sheba” Medical Center, Fax:
and as a result, wake periods occur at undesired
972-3-5349368. E-mail: [email protected]
times, therefore, the patient complains of insomnia
1087–0792/02/$-See front matter 2002 Published by Elsevier Science Ltd
or excessive daytime sleepiness. For most of the
Figures 1–3 display the rest-activity patterns of
CRSD, the major sleep episode is of normal duration
three patients suffering from Delayed Sleep Phase
with normal REM/NREM cycling, although in-
Syndrome, Non-24-h Sleep–Wake Syndrome and
termittent sleep episodes may occur in some dis-
Irregular Sleep–Wake Pattern, respectively. The
black areas represent activity, while the white ones
1. Delayed Sleep Phase Syndrome (DSPS): in this
disorder the major sleep episode is delayed in
CRSD CHARACTERISTICS
relation to the desired clock time resulting insymptoms of sleep-onset insomnia or difficulty
The pioneer report by Weizman et al. [5], published
in awakening at the desired time (Fig. 1).
in 1981, was followed by only a few studies, based
2. Advanced Sleep Phase Syndrome (ASPS): the
on small numbers of patients with no more than
major sleep episode is advanced in relation to
30 participants [6]. The only large study on CRSD
the desired clock time, resulting in symptoms of
patients [7] includes a survey of the characteristics
compelling evening sleepiness, early sleep onset,
of 322 patients suffering from CRSD and a case-
and an awakening that is earlier than desired.
control study comparing a group of 50 CRSD
3. Non-24-h Sleep–Wake Syndrome (Free-Running
patients and 56 age and sex matched normal sub-
pattern): consists of a chronic steady pattern
jects. The major findings were: a great majority
comprised of several hours daily delays in sleep
(84.6%) of the patients were found to have DSPS,
onset and wake times in an individual living in
12.3% had a Non-24-h Sleep Wake Syndrome, while
only a handful of patients were diagnosed with
4. Irregular Sleep–Wake Pattern (disorganized):
an Irregular Sleep–Wake Pattern (1.9%) and ASPS
consists of temporally disorganized and variable
(1.3%). In a report from a sleep clinic in Japan similar
episodes of sleep and waking behaviour (Fig. 3).
data was recorded [8]. The low prevalence of ASPS
5. Shift work and 6. jet lag that are beyond the
in CRSD may be due to fact that ASPS is a condition
that is better tolerated than DSPS. It is much easier
to keep oneself awake for a few hours after the
be 0.13% in Japan [9] 0.17% in Norway [10] and
habitual bed-time, than to force oneself to fall asleep
7.3% of adolescents in the western population [11].
a few hours before one’s habitual bed-time – a veryfrustrating if not an impossible task.
The majority of patients (89.6%) reported onset
BIOLOGICAL ASPECTS OF CRSD
of CRSD in early childhood or adolescence; no sexdifferences were evident; a familial trait existed in
CRSD patients differ from night or morning type
people (“owls” and “larks”) in the rigidity of their
The reported prevalence of CRSD in these stud-
maladjusted biological clock. While “owls” and
ies [7, 8] reflects the population of patients who
“larks” prefer morning or evening, they are flexible
approach sleep specialists for help. There is, at the
and can adjust to the demands of the environmental
present time, very limited data available regarding
clock. CRSD patients, on the other hand, appear
the prevalence of CRSD in the general population.
to be unable to change their clock by means of
The prevalence of the disorder was estimated to
Irregular (or Diosorganized) Sleep Wake Pattern.
In CRSD not only the sleep–wake cycles deviates
authors explain the patho-physiology of DSPS and
but also other circadian physiological rhythms such
the rigidity of their internal clock by these findings.
as: melatonin and body temperature [12–14]. The
Another study [14] compared the core body
involvement of several biological rhythms in this
temperature schedule of DSPS compared to normal
disorder may be a part of the explanation why is
controls. They found that sleep length and tem-
it so difficult for these patients to change their
perature nadir to sleep offset interval were sig-
sleep–wake schedule. Uchiyama et al. [15] looked
nificantly longer in DSPS than in the control group.
for the cause for the inability of CRSD patients to
They suggest, that the rigidity of DSPS patients’
reset sleep phase. They studied 11 DSPS patients
sleep–wake schedule is a result of their inability to
and 15 normal control in an ultra short sleep–wake
phase advance their temperature circadian clock, in
schedule measuring melatonin secretion in dim light
the same way that daily body temperature was
condition. DSPS patients failed to compensate for
identified as a physiological component in ad-
previous sleep loss compared to control subjects.
justment to shift work and jetlag [16].
Phase angle between sleep propensity rhythms and
Is the hereditary trend reported clinically re-
melatonin was wider in DSPS than in controls. The
flected in genetic studies also? A study investigated
the human leukocyte antigen (HLA) types A, B, and
Administration of B12 has been reported to
DR, of 42 DSPS patients and compared its frequency
normalize human sleep–wake rhythm disorders
with those of 117 healthy control subjects [17].
such as Non-24-h Sleep–Wake Syndrome, DSPS, or
Only HLA DR1 was significantly higher in DSPS,
insomnia. However, the mechanisms of the action
which indicates possible association between this
of B12 on the rhythm disorders are unknown [28].
antigen and DSPS and maybe the genetic factor for
It may act by changing the ocular receptors’ affinity
predisposition to DSPS. Others [18, 19] suggest
to light, or exert a direct influence on melatonin
that several mutations in the human melatonin 1a
[29], yet there is little experience with this treat-
[hMella] receptor gene are the cause of the bio-
ment and very few accounts appear in the literature.
All the reports of vitamin B12 efficiency for CRSDwere based on open studies, thus the effect ofvitamin B12 has not been accurately evaluated. DIAGNOSIS
There is only one double-blind study [30] evaluatingthe effect of 3 mg/day methylcobalamin or placebo
The best method to make the diagnosis of CRSD
administered for 4 weeks to DSPS patients. No
is by a clinical interview and a week of actigraphic
significant differences were observed between the
monitoring or sleep log in free conditions. Moni-
two groups in sleep–wake cycles and in the feeling
toring the sleep–wake schedule under forced con-
ditions can mask the pattern of the schedule thus
Light therapy, which became increasingly popular
misleading the diagnosis. The actigraph is a watch
as the importance of light in resetting the circadian
size device worn on the wrist sampling hand motion.
system was recognized, involves using morning
A computerized algorithm can provide highly re-
bright light exposure to induce a phase advance in
liable data on sleep and wake periods of the patient
both sleep onset and wake times [31]. Even very
[20, 21]. We believe that actigraphy is the best
short term (5 days) of phototherapy on six patients
objective diagnostic tool for CRSD, as opposed to
with DSPS proved advancement of sleep phase and
polysomnography (PSG), which is not an adequate
body minimum temperature [32]. Practice para-
tool for the assessment of CRSD. This is due to
meters for the use of light therapy in the treatment
the nature of CRSD, which requires monitoring for
of sleep disorders was published by the Standards
several days in order for the patients’ sleep–wake
of Practice Committee, American Academy of Sleep
pattern to manifest itself clearly. This is very difficult
Medicine [33]. They maintain that, light therapy has
to do with PSG, yet can be perfectly demonstrated
been found to be a useful treatment for DSPS and
by actigraphy (see Figs 1–3). Melatonin secretion
ASPS, but its benefits for the treatment of non-24-
and/or temperature measure for at least 36 hours
h sleep-wake syndrome, jet lag and shift work
every two hours can be an additional diagnostic
are less clear. However this treatment demands
30–60 min of sitting in front of a light-box everymorning or evening, which is complicated to managefor many DSPS patients. TREATMENT
While chronotherapy and light therapy are de-
manding and difficult treatments, which usually lead
Patients suffering from DSPS are treated with one
to compliance problems (thus giving rise to few
of, or a combination of several methods, such aschronotherapy [22], light therapy [23], vitamin B12
reports in the literature), melatonin administration,
[24], or melatonin administration [25, 26].
is a relatively simple and easy treatment option.
The term chronotherapy in sleep medicine refers
Studies have shown that melatonin has a sleep-
to a behavioral technique in which bedtime is sys-
promoting and entraining action when taken in the
tematically delayed, so following the natural tend-
evening. The effects of the administration of small
ency of human biology. This is done, until sleep
doses of melatonin (0.5–5.0 mg.) have been shown
onset time coincides with the desired sleep time,
to follow a phase-response curve that is nearly the
where the conventional 24-h day is re-established.
opposite of light curve [34]. Phase advances are
Consequently, the patient is advised to maintain the
produced by melatonin administered in the evening,
newly achieved bedtime rigidly, and from then on
while phase delays appear when it is administered
in the early morning [35]. It is also been shown
that melatonin induces temperature suppression
Dahlitz et al. [25] illustrated that an oral dose of
[36], and that there is a direct relationship between
5 mg of melatonin taken in the evening causes a
the ability of melatonin to phase shift the endo-
significant phase advance toward conventional times
genous circadian clock and its temperature sup-
of both sleep onset and awakening with no significant
pressing quality [37]. These characteristics seem to
changes in sleep duration or architecture. Oldani
be what makes melatonin an effective means of
et al. [51], treated six DSPS patients with 5 mg of
dealing with chronobiological disorders. In studies,
melatonin for a period of one month, with similarly
where only part of them were randomized placebo-
positive results, and no changes to sleep ar-
controlled, melatonin proved to be effective in: shift
chitecture or duration. In both studies, however,
work induced sleep disorders [38], sleep dis-
the pretreatment sleep pattern returned 2–3 days
turbances caused by a de-synchronization of the
endogenous sleep-wake cycle from lighting cues in
While the above studies all support the efficiency
blind, geriatric and brain damaged subjects [39]
of melatonin treatment for DSPS, they were all
CRSD, including DSPS [25, 26, 40]. In a double-
carried out on a relatively small number of DSPS
blind placebo-controlled cross-over study [41] the
patients. Over the past six years, over 400 people
effect of 5 mg melatonin administration to 25 DSPS
suffering from DSPS have been referred to our
patients was investigated. The influence of melatonin
sleep and chronobiology clinic. Most of these
was assessed by: 24-h melatonin and rectal tem-
patients were treated with melatonin based on
perature curve, polysomnography, actigraphy, sleep
the principles suggested by Dahlitz et al. [25], and
log and subjective sleep quality assessment. After
received guidelines regarding maintenance of their
treatment there was a significant advancement in
new sleep patterns. After a substantial period of
melatonin curve (approximately 1.5 h), actigraphic
time had elapsed, we decided to conduct a subjective
and PSG sleep onset and offset and people felt
follow-up study [26]. In this study, we attempted
more refreshed in the morning. The temperature
to investigate the effectiveness of the treatment
curve did not move significantly. Another study
and the existence of any possible side effects. We
comparing melatonin and placebo treatment for
also hoped to ascertain whether a relationship exists
DSPS confirmed these results [42]. Recently several
between the length of effectiveness of the treatment
studies reported on the effects of melatonin on the
and certain aspects of the illness. This study, which
quality of life of DSPS patients [43], for DSPS
accompanied routine treatment in our sleep clinic,
patients suffering from chronic headache [44] and
examined the efficiency of melatonin treatment in
for the regulation of CRSD of mentally retarded
a relatively large sample of DSPS subjects by means
children [45, 46]. There are controversies about its
of subjective reports. A sample of 61 subjects, 37
males, and 24 females were diagnosed with DSPS
It has been shown that melatonin has an ex-
by means of clinical assessment and actigraphy. Their
tremely wide margin of safety, at least in terms of
mean pre-treatment falling asleep and waking times
short-term side effects. In a study that examined
the effects of oral melatonin on skin color and the
98.58 min), respectively. They were treated with a
release of pituitary hormones, five patients with
six-week course of treatment comprising 5 mg of
hyper-pigmented skin were given 1 g/day of me-
oral melatonin taken daily at 22.00 h. Twelve to
latonin orally for a period of 30 days, with minimal
eighteen months after the end of the treatment, a
adverse effects. These patients did complain of
survey questionnaire was sent to the home of each
increased drowsiness, but a thorough examination
subject to investigate the efficiency of the melatonin
did not reveal any evidence of toxicity [49] despite
treatment and its possible side effects. 96.7% of the
the very high dosage used in this study (200–2000
patients reported that the melatonin treatment was
times greater than that generally used for the treat-ment of circadian disorders). It should be noted
helpful, with almost no side effects. Of these, 91.5%
that even a 0.5–5.0 mg dosage of melatonin is higher
reported a relapse to their pre-treatment sleeping
than normal nocturnal levels of melatonin in the
patterns within one year of the end of treatment.
blood. Moreover, Arendt points out that no data
Only 28.8% reported that the relapse occurred
exist on long-term studies in humans [50], therefore
within one week. The pre-treatment falling asleep
questions of safety have yet to be fully researched
and waking times of patients in whom the changes
were retained for a relatively long period of time
were significantly earlier than those of patients
CRSD patients, to which he or she has been sub-
whose relapse was immediate (t=2.18, P<0.05; t=
jected since early childhood or adolescence, adds
2.39, P<0.05, respectively), with no difference in
psychological distress to the practical difficulties of
sleep duration. There are CRSD patients for whom
coping with life. Several studies found depression
all these treatment modalities fail to help. In these
to be frequent in DSPS [6, 56, 57] Is it an outcome
cases it becomes a CRSD Disability [53] and the
of their failure to adjust to the environmental every-
only successful treatment is rehabilitation i.e. for
day life demands or simply symptoms of fatigue as
the patient to adopt a new career that enables
a result of ongoing partial sleep deprivation?
to work within the limits of his chronobiological
Attention Deficit Hyperactive Disorder (ADHD)
has also been found to be related to the instabilityof the sleep-wake system [58]. Thirty-eight school-age boys with ADHD and 64 controls were ex-amined with actigraphs and sleep diaries over five
CRSD IN PSYCHIATRY
consecutive nights. Discriminant analysis revealedthat children’s classification (ADHD versus control)
It has been found that there is a high prevalence of
could be significantly predicted on the basis of their
learning disorders (19.3%) and personality disorders
(22.4%) in people who have CRSD [7]. The high
prevalence of personality disorders in CRSD
characteristic of numerous psychopathologies such
patients has been confirmed in a controlled study,
as depression, anxiety, PTSD etc. We wish to em-
which found that individuals suffering from CRSD
phasize the fact that no existing psychopathology is
are characterized to a greater extent by personality
characterized by a sleep disorder of the circadian
disorders than a control group [54]. In a com-
plementary study [55] 63 hospitalized adolescentswere studied. None of them had any diagnosedmedical disorders, and all were being treated with
DRUG-INDUCED CRSD
psychiatric drugs. Ten subjects were diagnosed assuffering from DSPS according to a sleep–wake
Can pharmacological treatments cause CRSD as a
schedule structured interview. Subjects diagnosed
side effect? Wirz-Justice et al. [59], describe a case
as suffering from personality disorders had a sig-
of a patient with chronic schizophrenia, treated with
nificantly higher probability of also suffering from
haloperidol, and showing signs of CRSD. Changing
DSPS. Additional findings were that patients with
medication to clozapine showed a direct effect
DSPS were more likely to have received an DSM
on his sleep and established a more organized
IV axis II diagnosis only, and were more likely to
sleep–wake pattern. Another report [60] is of a 22
be diagnosed as suffering from a distinct group of
year-old male patient who was diagnosed at the age
disorders characterized by affective lability. The
of 16 as suffering from Tourette Syndrome and
findings of DSPS and personality disorders, may
severe OCD. The Tourette Syndrome has been
lend some support to the hypothesis that inborn
successfully treated with haloperidol for 6 years.
peculiarities in the sleep–wake rhythm lead to the
After 2 years of treatment with haloperidol he
social and functional difficulties characteristic of
began showing signs of disorganized sleep, which
clearly were not present before. The patient com-
Learning disorders and even personality disorders
plained of difficulties in falling asleep at a regular
are related or may even be an outcome of CRSD.
time and a severe problem in awakening at the
A child who does not get enough sleep at night will
desired time for daily activity. The problem has
not be alert during the day in school, and is prone
caused him severe difficulties in day-to-day func-
to have trouble keeping up with the other children.
tioning and due to this he was unable to keep a job
Frequently, the patients’ parents, teachers, doctors,
on a regular basis. He was a very talented computer
or psychologists believe that the patients’ biological
systems analyst and had started to work from home
sleep–wake problem and the accompanying dys-
function at school are motivational or psychological
A night of polysomnography revealed no sleep
in nature, a belief that during the years, the patients
apnea. Three weeks of actigraphy done in a free
tend to adapt themselves. This attitude toward
running condition showed a disorganized sleep–
wake schedule. The patient was taken off the hal-
minor [62]. This group is usually characterized as
operidol and was given risperidone 1 mg/day. He
suffering from Disorganized Circadian Rhythm Sleep
reported an improvement in his sleep difficulties
Disorder [DCRSD] with onset later than is common
and no worsening of his Tourette symptoms. A
for other types of CRSD. This is opposed to the
revised actigraphic monitoring confirmed the
findings of Quinto et al. [63], who described one
patient’s subjective feeling. Additional 5 mg oral
case of DSPS and not DCRSD occurring after brain
melatonin taken at 21.00 h was added to the
trauma and the findings of Negtegaal et al. [64]. In
risperidone and a full recovery was documented in
all the cases there were no objective pathological
a third follow-up actigraphy. This was accompanied
finds in imaging (CT, MRI or EEG), and no cognitive
by his feeling of a significant improvement. The
dysfunction, but patients complained of difficulty in
patient was unable to find enough superlatives to
falling asleep and waking up as well as sleepiness
describe the change in his life. After years of dif-
during the day. All of the patients had no complaints
ficulties in coping with his occupational and social
of sleep–wake cycle inconsistency previous to the
life due to unconventional sleep timing, he at last
trauma, but all of them had been misdiagnosed for
started to have an organized schedule that has
years following their injury. The diagnoses were
enabled him to recover his diurnal life.
often psychiatric in nature, and often mistreated
Is haloperidol the only psychiatric drug that can
pharmacologically. Some cases were given the psy-
provoke CRSD? Hermesh et al. [61] reported on
chological diagnosis of PTSD (Post-Traumatic Stress
ten patients who developed typical DSPS during
Disorder) although they did not meet the criteria
treatment with the specific SRI agent fluvoxamine
for PTSD. Many patients were just thought to be
(FVA), prescribed for their obsessive-compulsive
malingering in order to gain financially from their
disorder. The delay in falling asleep ranged between
2.5–4 h later than the patients’ normal sleep routine.
While treatment with melatonin is useful in DSPS,
In the first five patients, DSPS was initially mis-
it has been found to be little or no help in treating
diagnosed as FVA induced somnolence or sedation.
DCRSD following head trauma [62]. Since there is
The causal role of FVA in the development of DSPS
no effective pharmacological therapy, the approach
in this series is corroborated by several pieces of
to CRSD after head trauma should be rehabilitation
clinical evidence: FVA was the only drug taken by
[53]. As with any other disability following physical
these patients. In all patients, first appearance of
trauma, the patient must understand and accept
DSPS had occurred following FVA initiation. In all
that the disability is permanent and should be guided
10 cases, where FVA was withdrawn, or the dose
in overcoming it. The patient should be encouraged
considerably decreased, DSPS disappeared. Re-ex-
to consider changes in his daily lifestyle, possibly a
posure of 3 patients to FVA again led to the return
change of occupation that conforms more to the
of DSPS. No case of spontaneous remission of DSPS
hours he is awake, possibly, in certain cases, working
was observed, even when FVA was administered
from home, and setting his own timetable.
for longer than 2 years (range 5.5 weeks–2.2 years).
It is not yet clear why minor head trauma causes
Emergence of FVA-induced DSPS was not im-
the onset of CRSD. Possibly there is a micro damage
mediate, and at least 5 days of ingestion, with no
to the pathways that are responsible for the syn-
less than 100 mg/d of FVA, had passed before
chronization between internal and external clocks.
patients first notice the change in their normal sleep
It is also possible that this damage is the reason
pattern. The authors conclude that FVA can cause
why we are unable to treat DCRSD brought on by
DSPS, which is often overlooked by the clinician
head trauma successfully with melatonin.
or misdiagnosed as psycho-physiological insomnia. Additional treatment with melatonin 5 mg at 21.00 h
CONCLUSION
can re-organize the sleep–wake schedule of thesepatients thus enable to continue the FVA use.
CRSD are sleep pathologies rarely familiar to doc-tors. Many of our CRSD patients had, for years, been
CRSD AND HEAD TRAUMA
wrongly diagnosed by neurologists, pediatricians andespecially by psychiatrists as psycho-physiological
It has been found that certain people have developed
insomniacs, and therefore unsuccessfully treated,
CRSD after head trauma, even when the trauma is
usually with sleeping pills [7]. Early onset of CRSD,
the ease of diagnosis, the high frequency of mis-
Research Agenda
diagnosis and erroneous treatment, the potentially
1. The prevalence of CRSD in the general popu-
lation is yet unknown and requires a study.
sequences, and the availability of promising treat-
2. More has to be done in order to understand
ments, all indicate the importance of greater
the biological mechanisms involved in the de-
awareness of these disorders. Doctors from various
synchronization of CRSD patients biological
chiatrists, neurologists, as well as psychologists and
3. The hereditary trend of CRSD should point
teachers should be more alert to the existence of
to studies on the genetic basis of the disorder.
4. Are there more drugs for which CRSD is one
5. More research needs to be done on the safety
and efficacy of CRSD treatments, including
Practice Points
When patients complain of sleep difficulties thedoctor should ask some additional clinical ques-tions about their sleep–wake habits. ACKNOWLEDGEMENTS
If CRSD is suspected, we suggest asking some
The author is grateful to Mrs Judith Abadi for her
1. Hunger times: the patient should be ques-
tioned about his/her preferable eating hours– whether she/he eats or is hungry during the
REFERENCES
night, and whether she/he ever eats early inthe morning
1. Moore-Ede MC, Sulzman FM, Fuller CA. The clocks
2. Hours of alertness: DSPS patients, even when
that time us. Harvard University Press 1982.
they wake up early and should thus become
2. Czeisler CA, Kronauer RE, Allan JS, et al. Bright light
more and more tired as the day passes, will
induction of strong (type O) resetting of the human
paradoxically become more alert as evening
circadian pacemaker. Science 1989; 244: 1328.
3. Thorpy MJ, Diagnostic Classification Steering Com-
mittee, ICSD- International classification of sleep dis-
3. Heredity: patients should be asked about close
orders: Diagnostic and coding manual. Rochester, MN:
family members with the same characteristics.
American Sleep Disorders Association. 1990.
4. Functional difficulties: CRSD patients often
4. American Psychiatric Association. Diagnostic and
have trouble functioning in everyday life. The
Statistical Manual of Mental Disorders, Fourth Edition.
hallmark of their problem is a severe difficulty
Washington, DC, American Psychiatric Association.
5. Rigidity of the biological rhythm: CRSD
∗5. Weitzman ED, Czeisler CA, Coleman RM, Spielman
patients have very rigid biological clocks.
AJ, Zimmerman JC, Dement W. Delayed sleep phase
Therefore, it is extremely difficult for them
syndrome. Arch Gen Psychiatry 1981; 38: 737–746.
6. Regestein QR, Monk TH. Delayed sleep phase
to adjust to environmental demands, even for
syndrome: A review of its clinical aspects. Am J
a very limited time. They should be asked
Psychiatry 1995; 152(4): 602–608.
about their sleep-wake habits during vacation
∗7. Dagan Y, Einstein M. Circadian rhythm sleep dis-
orders: towards a more precise definition and
6. Head Injury: patients displaying symptoms of
diagnosis. Chronobiology International 1999; 6(2):
an Irregular Sleep–Wake Schedule should be
8. Kamei Y, Urata J, Uchiyaya M, Ozaki S, Shibui
K, Okawa M. Clinical characteristics of circadian
7. Drugs side-effect: It is advised for psychiatrists
rhythm sleep disorders. Psychiatry Clin Neurosci 1998;
treating patients with psychotropic drugs to
52(2): 234–235.
take into consideration CRSD as a possibleside effect of this group of drugs.
∗ The most important references are denoted by an asterisk.
9. Yazaki M, Shirakawa S, Okawa M, Tagahashi K,
actigraphy in the evaluation of sleep disorders. Sleep
Demography of sleep disturbances associated with
1995; 18(4): 288–302.
circadian rhythm sleep disorders in Japan. Psychiatry
22. Czeisler CA, Richardson GS, Coleman RM, Zim-
Clin Neurosci 1999; 53: 267–268.
merman, JC; Moore-Ede, MC; Dement, WC; Weitz-
10. Schrader H, Bovin G, Sand T. Delayed and advanced
man, ED. Chronotherapy: Resetting the circadian
sleep phase syndromes. J Sleep Res 1993; 2: 51–55.
clocks of patients with delayed sleep phase in-
11. Paleo RP, Thorpy MJ, Glovinsky P. Prevalence of
somnia. Sleep 1981; 4(1): 1–21.
delayed sleep phase syndrome among adolescents.
23. Lewy AJ, Sack RL. Light therapy and psychiatry. Sleep Res 1998; 17: 391. Proceedings of the Society for Experimental Biology and
12. Shibui K, Uchiyama M, Okawa M. Melatonin
Medicine 1986; 183: 11–18.
rhythms in delayed sleep phase syndrome. J Biol
24. Okawa M, Mishima K, Nanami T, Shimizu T, Iijima
Rhythms 1999; 14(1): 72–76.
S, Hishikawa Y, Takahashi K. Vitamin B12 treatment
∗13. Oren DA, Turner EH, Wehr TA. Abnormal cir-
for sleep-wake rhythm disorders. Sleep 1990; 13(1):
cadian rhythms of plasma melatonin and body tem-
peratures in the delayed sleep phase syndrome. J
∗25. Dahlitz M, Alvarez B, Vignau J, English J, Arendt J,
Neurol Neurosurg Psychiatry 1995; 55(8): 665–70.
Parkes JD. Delayed sleep phase syndrome response
14. Ozaki S, Uchiyama M, Shirakawa S, Okawa M.
to melatonin. Lancet 1991; 337(8750): 1121–1124.
Prolonged interval from body temperature nadir
∗26. Dagan Y, Yovel I, Hallis D, Einstein M, Raichik I.
to sleep offset in patients with delayed sleep phase
Evaluating the role of melatonin in the long-term
syndrome. Sleep 1996; 19(1); 36–40.
treatment of DSPS. Chronobiology International 1998;
∗15. Uchiyama M, Okawa M, Shibui K, Lui X, Hayakawa
15(2): 181–190.
T, Kamei T, Takahashi K. Poor compensatory func-
27. Roehrs T, Roth T. Chronic insomnias associated
tion for sleep loss as a pathogenic factor in patients
with circadian rhythm sleep disorders. In: Kryger
with delayed sleep phase syndrome. Sleep 2000;
MH, Roth T, Dement WC, Eds. Principles and
23(4): 553–558.
Practice of Sleep Medicine. Philadelphia: W. B. Saun-
16. Kruger MH, Roth T, Dement WC. Principals and
Practice of Sleep Medicine. 3rd ed. Pennsylvania:
28. Ebihara S, Mano N, Kurono N, Komuro G, Yosh-
imura T. Vitamin B12 affects non-photic entrainment
17. Hohjoh H, Takahashi Y, Hatta Y, Tanaka H, Akaza
of circadian locomotor activity rhythms in mice.
T, Tokunaga K, Honda Y, Juji T. Possible association
Brain Research 1996; 15: 727(1–2): 31–39.
of human leucocyte antigen DRI with delayed sleep
29. Mayer G, Kroger M, Meier-Ewert K. Effects of
phase syndrome. Psychiatry Clin Neurosci 1999; 53(4):
vitamin B12 on performance and circadian rhythm
in normal subjects. Neuropsychopharmacology 1996;
18. Ebisawa T, Kajimura N, Uchiyama M, Katoh M,
15(5): 456–464.
Sekimoto M, Watanabe T, Ozeki Y, Ikeda M, Jodoi
30. Okawa M, Takahashi K, Egashira K, Furuta H, Hi-
T, Sugishita M, Iwase T, Kamei Y, Kim K, Shibui
gashitani Y, Higuchi T, Ichikawa H, Ichimaru Y.
K, Kudo Y, Yamada N, Toyoshima R, Okawa M,
Vitamin B12 treatment for delayed sleep phase
Takahashi K, Yamauchi T. Alleic variants of human
syndrome: A multi-center double-blind study. Psy-
melatonin 1a Receptor: Function and prevalence in
chiatry Clin Neurosci 1997; 51(5): 275–279.
subjects with circadian rhythm sleep disorders.
31. Weyerbrock A, Timmer J, Hohagen F, Berger M,
Biochem Biophys Res Commun 1999; 262(3): 832–
Bauer J. effects of light and chronotherapy on human
circadian rhythms in delayed sleep phase syndrome:
19. Ebisawa T, Uchiyama M, Kajimura N, Kamei Y,
cytokines, cortisol, growth hormone and sleep-
Shibui K, Kim K, Kudo Y, Iwase T, Sugishita M,
wake cycle. Biol Psychiatry 1996; 40(8): 794–797.
Jodoi T, Ikeda M, Ozeki Y, Watanabe T, Seklimoto
32. Watanabe T, Kajimura N, Kato M, Sekimoto M,
M, Katoh M, Yamada N, Toyoshima R, Okawa M,
Takahashi K. Effects of phototherapy in patients
Takahashi K, Yamauchi T. Genetic polymorphisms
with delayed sleep phase syndrome. Psychiatry Clin
of human melatonin 1b receptor gene in circadian
Neurosci 1999; 53(2): 231–233.
rhythm sleep disorders and controls. Neurosci Lett
∗33. Chesson AL Jr, Littner M, Davila D, Anderson WM,
2000; 280(1): 29–32.
Grigg-Damberger M, Hartse K, Johnson S, Wise M.
20. Sadeh A, Aesler DU, Lawre P. Actigraphically based
Practices and parameters for the use of light therapy
automatic bedtime sleep-wake recording: Validity
in the treatment of sleep disorders. Standards of
and clinical applications. J of Ambulatory Monitoring
Practice Committee, American Academy of Sleep
1989; 2: 209–216.
Medicine. Sleep 1999; 22(5): 641–660.
21. Sadeh A, Hauri PJ, Kripke DF, Lavie P. The role of
34. Skene DJ, Lockley SW, Arendt J. Use of melatonin
in the treatment of phase shift and sleep disorders.
double-blind trial. Am J Psychiatry 1999; 156(9): Adv Exp Med Biol 1999; 467(48): 79–84.
35. Sack RL, Lewy AJ. Melatonin administration phase
49. Norlund JJ, Lerner AB. The effects of oral melatonin
advances endogenous rhythms in humans. Sleep
on skin color and on the release of pituitary hor-
Research 1988; 17: 396.
mones. J Clin Endocrinol Metab 1977; 45(4): 768–774.
36. Cagnacci A, Elliot JA, Yen SS. Melatonin: A major
∗50. Arendt J. Melatonin: Claims made in the popular
regulator of the circadian rhythm of core tem-
media are mostly nonsense. BMJ 1996; 312: 1242–
perature in humans. J Clin Endocrinol Metab 1992;
75(2): 447–452.
51. Oldani A, Ferini-Strambi L, Zucconi M, Stanov B,
Fraschini F, Smirne S. Melatonin and delayed sleep
∗37. Deacon S, Arendt J. Melatonin-induced tem-
phase syndrome: Ambulatory polygraphic evalu-
perature suppression and its acute phase-shifting
ation. Neuroreport 1994; 6(1): 132–134.
effects correlate in a dose-dependent manner in
52. Alvarez B, Dahlitz MJ, Vignau J, Parkes JD. The
humans. Brain Research 1995; 688(1–2): 77–85.
delayed sleep phase syndrome: clinical and in-
38. Folkard S, Arendt J, Clark M. Can melatonin im-
vestigative findings in 14 Subjects. Journal of Neur-
prove shift worker’s tolerance of the night shift?
ology, Neurosurgery and Psychiatry 1992; 55: 665–670.
Some preliminary findings. Chronobiol Int 1993;
53. Dagan Y, Abadi J. Sleep Wake Schedule Disorder
10(5): 315–320.
(SWSD) Disability - A biological rhythm untreatable
39. Jan JE, Espezel H, Appleton, RE. The treatment
pathology. Chronobiol Int (in press).
of sleep disorders with melatonin. Developmental
54. Dagan Y, Sela H, Omer H, Hallis D, Dar R. High
Medicine and Child Neurology 1994; 36: 97–107.
prevalence of personality disorders among circadian
40. Lewy AJ, Ahmed S, Sack RL. Phase shifting in the
rhythm sleep disorders (CRSD) patients. Journal of
human circadian clock using melatonin. Behav BrainPsychosomatic Research 1996; 41(4): 357–363. Res 1996; 73(1–2): 131–134.
55. Dagan Y, Stein D, Steinbock M, Yovel I, Hallis D.
∗41. Nagtegaal JE, Kerkhof GA, Smits MG, Swart AC,
Frequency of delayed sleep phase syndrome among
van der Meer YG. Delayed sleep phase syndrome:
hospitalized adolescent psychiatric patients. Journal
A placebo-controlled cross-over study on the ef-
of Psychosomatic Research 1998; 45: 15–20.
fects of melatonin administered five hours before
56. Schrader H, Bovim G, Sand T. Depression in the
the individual dim light melatonin onset. J Sleep Res
delayed sleep phase syndrome. Am J Psychiatry 1996;
1998; 7(2): 135–143. 153(9): 1238.
42. Skene DJ, Lockley SW, Arendt J. Use of melatonin
57. Kayumov L, Zhdanova IV, Shapiro CM. Melatonin,
in the treatment of phase shift and sleep disorders.
sleep and circadian rhythm disorders. Semin ClinAdv Exp Med Biol 1999; 467: 79–84. Neuropsychiatry 2000; 5(1): 44–55.
43. Nagtegaal JE, Laurant MW, Kerkhof GA, Smits MG,
58. Gruber R, Sadeh A, Raviv A. Instability of sleep
van der Meer YG, Coenen AM. Effects of melatonin
patterns in children with attention-deficit/hy-
on the quality of life in patients with delayed sleep
peractivity disorder. J Am Acad Child Adolesc Psy-
phase syndrome. J Psychosom Res 2000; 48(1): 45– chiatry 2000; 39(4): 495–501.
59. Wirz-Justice A, Cajochen C, Nussbaum P. A schizo-
44. Nagtegaal JE, Smits MG, Swart AC, Kerkhof GA,
phrenic patient with an arrhythmic circadian rest-
van der Meer YG. Melatonin-responsive headache
activity cycle. Psychiatry Res 1997; 73: 83–90.
in delayed sleep phase syndrome: preliminary ob-
60. Dagan Y. Sleep wake sleep disorders as a possible
servations. Headache 1998; 38(4): 303–307.
side effect of CNS medications. Chronobiol Int 1998;
45. Pillar G, Shahar E, Peled N, Ravid S, Lavie P, Etzioni
16(supp1): 25.
A. Melatonin improves sleep-wake patterns in psy-
61. Hermesh H, Lemberg H, Abadi J, Dagan Y. Circadian
chomotor retarded children. Pediatr Neurol 2000;
rhythm sleep disorders (CRSD) as a possible side
23(3): 225–228.
effect of fluvoxamine. CNS Spectrums 2001; 6(6):
46. Jan MM. Melatonin for the treatment of handicapped
children with severe sleep disorders. Pediatr Neurol
62. Dagan Y. Circadian rhythm sleep disorders following
2000; 23(3): 229–232.
head trauma. Sleep Research 1995; 24: 327.
47. Petrie K, Conaglen JV, Thompson L, Chamberlain
63. Quinto C, Gellido C, Chokroverty S, Masdeu J.
K. Effect of melatonin on jet lag after long haul
Posttraumatic delayed sleep phase syndrome. Neur-
flights. BMJ 1989; 298(6675): 705–707. ology 2000; 54(1): 250–252.
48. Spitzer RL, Terman M, Williams JB, Terman JS,
64. Nagtegaal JE, Kerkhof GA, Smits MG, Swart AC,
Malt UF, Singer F, Lewy AJ. Jet lag:clinical features,
van der Meer YG. Traumatic brain injury-associated
validation of a new syndrome-specific scale, and
delayed sleep phase syndrome. Funct Neurol 1997;
lack of response to melatonin in a randomized,
12(6): 345–348.
Psychology and Christian Counseling I. Introduction and Review. (55 minute segments) A. A Breakdown in Society - The Religion of Secular Humanism. 1. Until 100 years ago: Xn ethics=moral basis Western Society. 2. Now Secular humanism: man looks to himself for answers: Pr. 14:12 There is a way that seems right to a man, but its end is the way of death. 3. Theology replaced by social
Empirical Guidance on the Management of Infection in Primary Care in adults Aims ♦To provide a simple, best guess approach to the treatment of common infections. ♦To minimise the emergence of bacterial resistance in the community ♦ To promote the safe, effective and economic use of antibiotics Principles of treatment 1. This guidance is based on the best available evidence
 Sleep Medicine Reviews, Vol. 6, No. 1, pp 45–55, 2002
doi:10.1053/smrv.2001.0190, available online at http://www.idealibrary.com on
MEDICINE
Sleep Medicine Reviews, Vol. 6, No. 1, pp 45–55, 2002
doi:10.1053/smrv.2001.0190, available online at http://www.idealibrary.com on
MEDICINE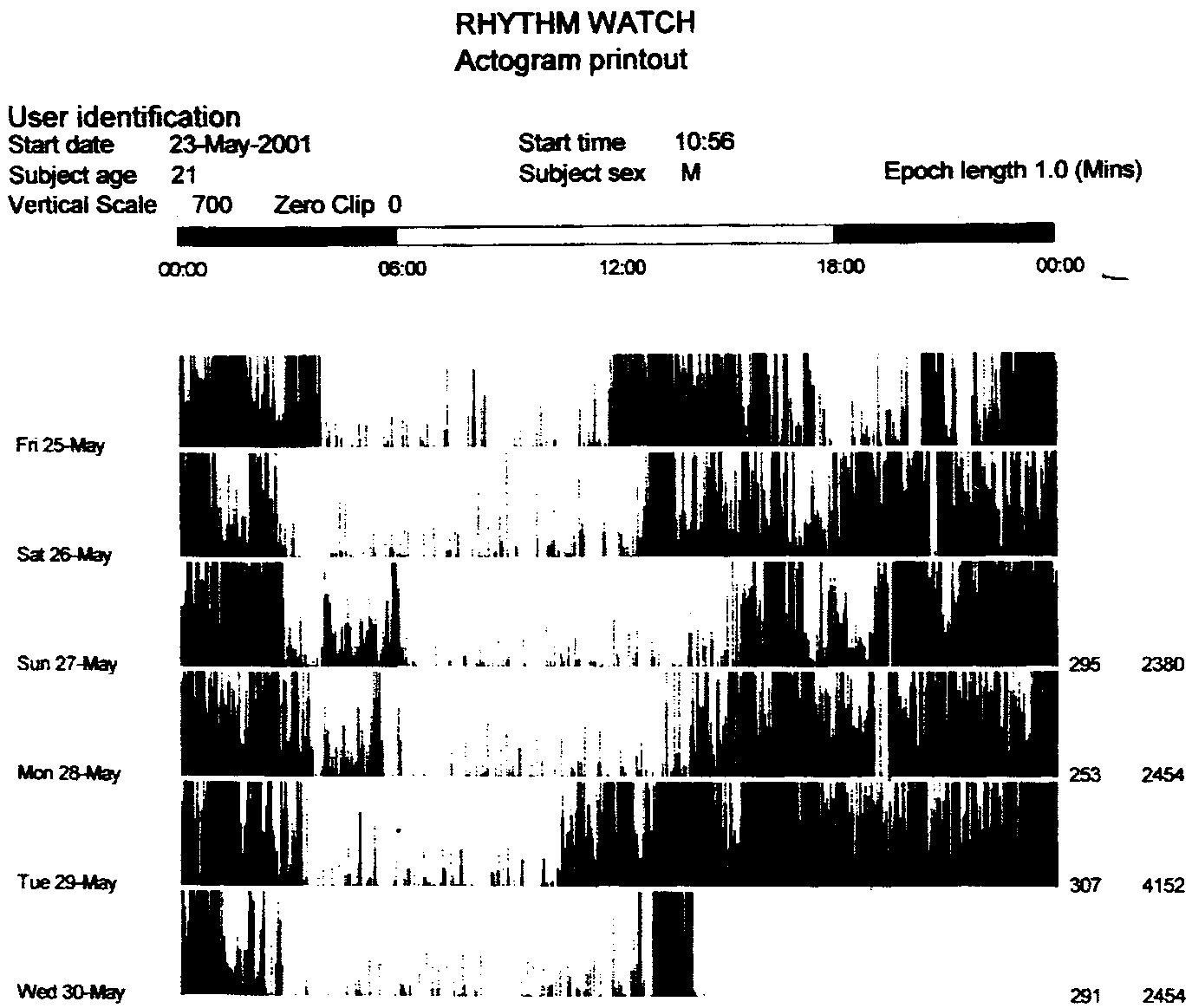 or excessive daytime sleepiness. For most of the
Figures 1–3 display the rest-activity patterns of
CRSD, the major sleep episode is of normal duration
three patients suffering from Delayed Sleep Phase
with normal REM/NREM cycling, although in-
Syndrome, Non-24-h Sleep–Wake Syndrome and
termittent sleep episodes may occur in some dis-
Irregular Sleep–Wake Pattern, respectively. The
black areas represent activity, while the white ones
1. Delayed Sleep Phase Syndrome (DSPS): in this
disorder the major sleep episode is delayed in
CRSD CHARACTERISTICS
or excessive daytime sleepiness. For most of the
Figures 1–3 display the rest-activity patterns of
CRSD, the major sleep episode is of normal duration
three patients suffering from Delayed Sleep Phase
with normal REM/NREM cycling, although in-
Syndrome, Non-24-h Sleep–Wake Syndrome and
termittent sleep episodes may occur in some dis-
Irregular Sleep–Wake Pattern, respectively. The
black areas represent activity, while the white ones
1. Delayed Sleep Phase Syndrome (DSPS): in this
disorder the major sleep episode is delayed in
CRSD CHARACTERISTICS to keep oneself awake for a few hours after the
be 0.13% in Japan [9] 0.17% in Norway [10] and
habitual bed-time, than to force oneself to fall asleep
7.3% of adolescents in the western population [11].
to keep oneself awake for a few hours after the
be 0.13% in Japan [9] 0.17% in Norway [10] and
habitual bed-time, than to force oneself to fall asleep
7.3% of adolescents in the western population [11].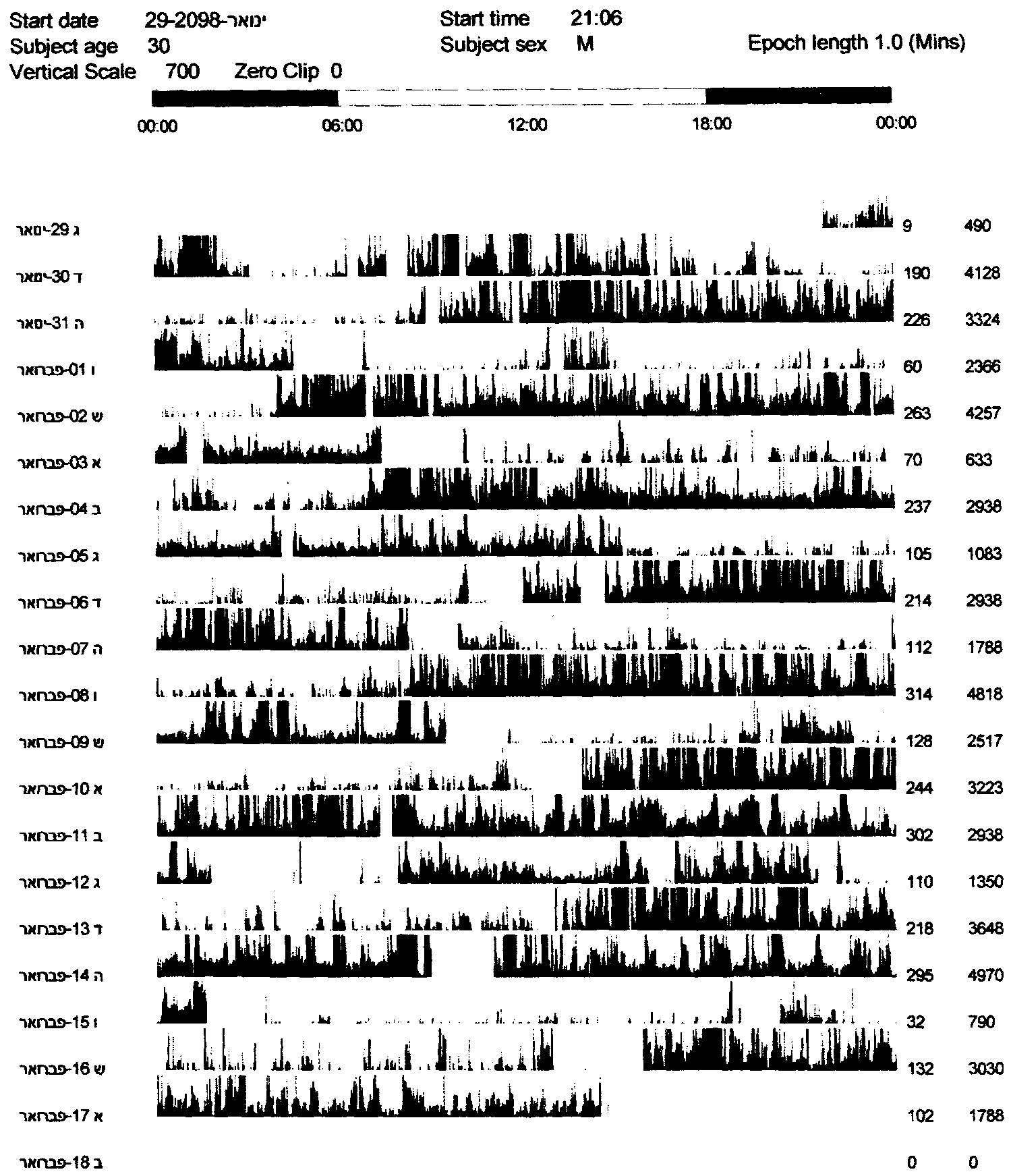 Irregular (or Diosorganized) Sleep Wake Pattern.
Irregular (or Diosorganized) Sleep Wake Pattern.