ME-CDMS-302a Revision 0 Approved by Approval Date 6/7/07 Active Divisions/Departments Active Division/Departments: Medical, McMurdo, South Pole, and Christchurch Raytheon Polar Services Company Medical Contract No. OPP 0000373 Hard Copy Not Controlled—Controlled Copy Available On-line McMurdo, South Pole, Christchurch, Denver Table of Contents
Procedure .1 References.2 Attachment 1, USAP Air Evacuation Mission Information .3 Attachment 2, McMurdo Hospital Standing Orders for Medevac Patients .4 Attachment 3, Routine Aeromedical In-Flight Kit .6 Attachment 4, Patient Classification.7 Attachment 5, AE Patient Preparation Checklist (Minimum Requirements) .8
Raytheon Polar Services Company Medical Department Contract No. OPP 0000373 Hard Copy Not Controlled—Controlled Copy Available On-line McMurdo, South Pole, Christchurch, Denver Procedure
1. Reference RPSC Procedure ME-CDMS-302, Patient Transport and Medical Evacuation
2. USAP Lead Physician will initiate the patient transfer in accordance with NSF/USAP
3. Use the standardized Patient Movement Precedence (JP 4-02.2 and AMCPAM 11- 303,
para 4.3) for category of patient severity.
a. Routine / Patient transfer – Ambulatory patient / litter on request or regular
aircraft seating, attendant may or may not be needed. Medical equipment or medications as required for specific medical problem, medical condition not expected to change in 72 hours
b. Priority - Litter patient, Oxygen available, possible cardiac monitor, routine
standardized AeroMed In-flight kit, one attendant (consider 2 attendants for cardiac patients), medications as required, medical condition could deteriorate in 24 hours
c. Urgent – Litter patient, oxygen required, cardiac monitor, routine standardized
Aero Med in-flight Kit + appropriate additional supplies, medications, two attendants as required, medical condition critical - immediate movement to save life, limb, eye sight.
4. USAF Flight Surgeon will call TPMRC at 13th AF in Hawaii and provide telephone
notification IAW Annex Q of JTF SFA CONOPS/Operation Deep Freeze. Use outline in attachment 1. Call 791-1-808-448-1602, wait for dial tone, and then #55722643 (use the # key).
5. USAF Flight Surgeon will call the 64AW/CC or OPS desk in Christchurch and provide a
report on the proposed Air Evac. Use the outline from Attachment 1 as per AMCPAM 11-303. Call 798 – (wait for tone) – (press # key to start) #697709 – (wait for tone) – 027-229-9384 (64 AW/CC) or 027-229-9287 (64 AW/Maintenance CC).
6. Fax a copy of a completed Attachment 1 to the 64AW – FAX to 798 – tone - #697709 –
7. Complete a copy of the USAP Medevac Orders and send with patient. See Attachment 2.
8. Review AMCPAM 11-303, paragraph 3.3 and assure that the appropriate equipment is
available for the transport. (See Attachment 3).
9. When possible, accompany the patient to Pegasus Field for transfer to the C-17.
Raytheon Polar Services Company Medical Department Contract No. OPP 0000373 Hard Copy Not Controlled—Controlled Copy Available On-line McMurdo, South Pole, Christchurch, Denver
10. Before placing the patient on the aircraft, hold a preflight briefing with the aircrew to
review expectations of patient care, special needs and significant medical issues for the flight. Have the accepting crew member sign the forms to document that the briefing has taken place. Assist the flight nurse and aircrew as appropriate in setting up the patient for the mission.
11. Hold a de-brief session upon Air Evac Team return to assess any transfer issues, enroute
medical problems and overall systems issues. Report any significant problems to USAP Lead Physician, JTF Deployed Commander and 64AW/CC for correction.
References
RPSC Procedure ME-CDMS-302, Patient Transport and Medical Evacuation Procedures Raytheon Polar Services Company Medical Department Contract No. OPP 0000373 Hard Copy Not Controlled—Controlled Copy Available On-line Attachment 1 USAP AIR EVACUATION MISSION INFORMATION DATE: _____________ MISSION INFORMATION (One patient per page): NOTE: If the political/operational climate is such that information below cannot be given, inform the TPMRC. 1. INDIVIDUAL ANNOTATING INFORMATION AND PHONE NUMBER: _________________________________________________________________________
McMurdo Clinic 720-568-1048 (From the US); e-mail: [email protected] 2. REFERRING PHYSICIAN: ___________________________________________ 3. HOSPITAL/CLINIC NAME: McMURDO STATION HOSPITAL 4. PATIENT’S NAME / RANK: _____________________________________________ 5. PATIENT’S SSN: ______________________________ 6. PATIENT’S COMMAND AND ORGANIZATION: (RPSC) (NSF) (GRANTEE) (T-Event) (ANG) (US MILITARY) (NZ) 7. NATURE OF INJURY: __________________________________________________ 8. DIAGNOSIS: __________________________________________________________ 9. VITAL SIGNS: SpO2 _____% Temp ______ Pulse _______ Resp______ B/P______ 10. PATIENT EQUIPMENT REQUIRED FOR MISSION: _______________________________________________________________________ 11. MEDICAL AUGMENTATION PERSONNEL REQUIRED: Y / N 12. CATEGORY: ______________________________________________ 13. REQUESTED MOVEMENT DATE: ___________________________ 14. DESTINATION: (MCMURDO STATION) (CHRISTCHURCH) (OTHER) 15. REQUESTED AIRFIELD FOR PICK-UP: (PEGASUS) (WILLIAMS FIELD)
16. OTHER CONTACTS, IF ANY: USAP MEDICAL COORDINATOR, CHRISTCHURCH, NZ, 798 - #699020 – 0274-714-282 17. TPMRPC NOTIFIED (Name, date and time):_______________________________ This message contains FOR OFFICIAL USE ONLY (FOUO) information which must be protected under the Privacy Act and AFI 33-332. The information contained in this E-mail message is privileged and confidential information intended only for the use of the SFA FLIGHT SURGEON or entity named above. If the reader of this message is not the intended recipient, you are hereby notified that any reading and dissemination, distribution, or copying of this communication i
ited. If you have received this communication in error,
please notify the SFA Flight Surgeon immediately by telephone at
Attachment 2 MCMURDO HOSPITAL STANDING ORDERS FOR MEDEVAC PATIENTS
Date: _____________ Pt Name/DOB: ______________________________________ Allergies: __________________________________________ □
Pulse Oximetry, apply oxygen PRN to keep SpO2 > 93% (prefer humidified)
IVF: _____________________ @ ________ ml/hr
Tylenol 650 mg /1000mg every 4-6hrs PRN (max 4G/day)
Morphine 2-5mg IV every 10 minutes for pain if SBP >100, resp rate >12.
(if allergy to Morphine:___________________________________________)
Narcan 0.4mg IV if resp rate <8/min and/or SpO2 < 90% with supplemental O2
Ativan 1 mg po/IV for anxiety every 6 hrs PRN
Prochlorperazine (Compazine) 5-10mg IV/IM every 6-8 hrs PRN nausea
Promethazine (Phenergan) 25mg IM/IV every 4-6 hrs PRN nausea
Benadryl 25-50mg IV/IM for extrapyramidal effects of Compazine/allergic
IV antibiotics: (please right out orders) ____________________________________________________________________________________________________________________________________
Oral Intake: Regular diet____ Soft Diet____ Clear Liquids______
NasoGastric Tube to: Continuous Suction_____ Intermittent Suction_______
□ Foley catheter to gravity drainage □
Activity: Confined to litter_____ May ambulate with Assist____
Bathroom Privileges: Bedside_____ With Assist____ Independent_____
If chest pain: □
NTG 1 spray SL every 5 minutes x 3; keep SBP >90. (IF NO VIAGRA IN THE LAST 24 HOURS) –if no relief of chest pain, then:
Nitroglycerin drip – start at 10mcg/min, titrate by 5-10mcg every 5 minutes until
Nitropaste 1inch to chest wall every 8 hours for CP not resolved with SL NTG.
If no relief with NTG, use morphine 2-5mg every 10 minutes for CP.
□ Follow ACLS protocols for cardiac arrest conditions. Please list all other orders pertinent to patient condition: ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ Provider Signature: _______________________________
Attachment 3
ROUTINE AEROMEDICAL IN-FLIGHT KIT 1. Life-Pak 12 Cardiac Monitor and Defibrillator 2. Life-Pak 12 Battery Support System 3. Portable Suction unit 4. Pulse Oxymeter 5. Oxygen Source - Certified "H" tank for C-130, PT-Lox Liquid Oxygen unit, or Internal Oxygen System for the C-17 6. Frequency Converter (for aircraft lacking 115 VAC/60Hz power source) 7. IV Infusion Pump 8. Electrical cable assembly set / extension cords 9. Ambu-bag with Oxygen connector 10. Intubation Kit 11. Emergency Medications 12. ACLS medication and equipment (List per AMCPAM 11-303, 3Nov2000)
Attachment 4
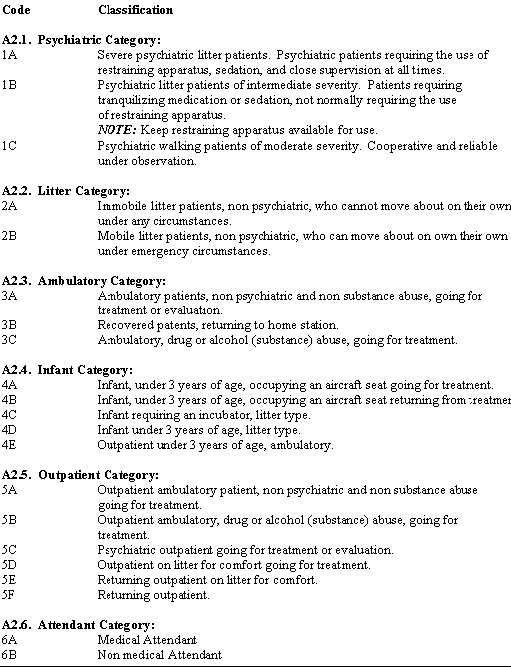
PATIENT CLASSIFICATION Attachment 5
AE PATIENT PREPARATION CHECKLIST (MINIMUM REQUIREMENTS)
A. DOCUMENTS TO ENTER PATIENT INTO DMRIS
AF Form 3839 or USAP Mission Information Data Collection Sheet ___________
B. DOCUMENTS REQUIRED TO ACCOMANY PATIENT FOR AE AF Form 3899 or USAP Air Evacuation Orders ------------------------------------___________ Anti-Hijacking Certificate ------------------------------------____________ Medical/Nursing Inpatient Transfer Summary ------------------------------------___________ Travel Orders (Military patient) -----------------------------------____________ Medical Records as required
-----------------------------------____________
--------------------------------------- ____________
----------------------------------------____________
----------------------------------------____________
AF Form 3838 for DNR patient ----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
DD Form 2239 Consent for Medical Care in the AE System -------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
Other Supplies as Requested by Physician ----------------------------------------____________
Destination as confirmed in the Mission Data Sheet ----------------------------- ____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
----------------------------------------____________
--------------------------------------- ____________
----------------------------------------____________
Availability of Flight Insurance/ Health Insurance
-----------------------------____________
----------------------------------------____________
Operational Discount Amendment Terms and ConditionsPT Coach Role is an exciting transitional role geared to assist the driven individual who is looking to make the transitioninto running their own Personal Training business. The PT coach role extends the otherwise 6 week apprentice period to up to 6 months long. It allows you to build your business gradually by engaging members using the curr
POLICIES ADOPTED 1986 The Conservation of Canada’s Arctic HeritageImproved Follow-Up of the Auditor General’s Annual Report EMERGENCY RESOLUTIONS Emergency Resolution: Women in Conflict with the LawEmergency Resolution: Funding Cuts to Studio ‘D’Emergency Resolution: Cabooseless Freight TrainsEmergency Resolution: Tobacco Marketing BoardEmergency Resolution: Legalization of the
 Attachment 4
Attachment 4