Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Microsoft word - document5
Case study: Woman presents with neovascular glaucoma Because panretinal photocoagulation was not an option in this patient, endoscopic pars plana vitrectomy was performed. By Robert F. Haverly, MD, FACS A 70-year-old woman was referred to me with neovascular glaucoma.
Her medical history was significant for hypertension and asthma. She was taking Vasotec (enalapril maleate, Merck), Advair (fluticasone propionate and salmeterol, GlaxoSmithKline) and albuterol. She had an ocular history of cataract extraction with posterior chamber IOL implantation in 1987 and
Robert F.
argon laser trabeculoplasty in both eyes in 1994. The patient had scarring of
her right cornea from a corneal ulcer in 2006.
In 2008, the patient developed a central retinal vein occlusion in her right eye. Shortly thereafter, vascularization of the iris could be visualized. The referring ophthalmologist performed panretinal photocoagulation, which was incomplete because of the poor view into the eye. The referring ophthalmologist also gave an Avastin (bevacizumab, Genentech) injection to the affected eye. The IOP was temporarily controlled with these maneuvers along with Azopt (brinzolamide ophthalmic, Alcon) twice daily in both eyes, Lumigan (bimatoprost ophthalmic solution 0.03%, Allergan) in both eyes every night at bedtime and Alphagan (brimonidine 0.1%, Allergan) twice daily in both eyes. However, the IOP elevated with time.
When I saw the patient, the IOP was 68 mm Hg and the patient was in pain. The patient also experienced a decrease in vision from counting fingers to hand motion. The cornea, iris and angle had vascularized and there was blood in the angle. There was a very poor view into the eye due to corneal scarring, edema and poor dilation from iris synechiae. Gonioscopy was difficult but revealed impressive vessels in the angle. The posterior chamber IOL was in good position, but with white lens material barely visible just posterior to the lens optic. The view of the retina was hazy because of the cornea and small pupil, and there was a mild vitreous hemorrhage (Figure 1). Panretinal photocoagulation could not be performed.
Figure 1. This is the patient’s eye with neovascular glaucoma showing significant corneal scarring and vascularization. Phenylephrine 2.5% and tropicamide 1% were placed prior to the photograph. Note the poor pupillary dilation secondary to the lens-iris synechiae and the large vessels associated with rubeosis.
Would you perform a transscleral cycloablative procedure? Would you perform a transscleral cycloablative procedure and place a glaucoma
Would you surgically dilate the pupil, perform a pars plana vitrectomy (PPV), and
Would you perform an endoscopic vitrectomy with endolaser of the retina and
Surgical course
After discussing the treatment options with the patient, I performed an endoscopic pars plana vitrectomy with endolaser of the retina and of the ciliary body. The view was not clear enough to visualize the retina through the cornea, so an endoscopic approach was necessary.
The endoscope with the endolaser cyclophotocoagulation (ECP) system (Endo Optiks) is ideal to assist with this type of vitrectomy. It can be performed through an opaque cornea and avoids having to stretch and dilate a rubeotic pupil. I used the 23-gauge vitrectomy system (Alcon). A 23-guage infusion port was placed in the inferior temporal quadrant and a 23-gauge sleeve was placed in the superior temporal quadrant. A larger 19-gauge sclerostomy was made in the superior nasal quadrant. A 19- to 20-gauge port is necessary to insert the endoscopic laser. With the infusion on in the inferior port, the straight
endoscope was placed through the 19-gauge opening. The Occutome (Alcon) was placed in the superior temporal port and a complete vitrectomy was performed (Figure 2). As the vitreous base was removed, several pieces of white lens material fell onto the macula. The lens remnants were located with the endoscope and removed with the Occutome. At times, the endoscopic probe tip was used to help move and crush the lens material into the Occutome.
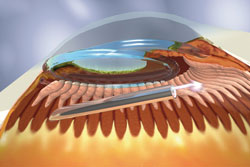
Figure 2. The endoscopic Figure 3. The endoscopic probe is shown probe is on the right through ablating the ciliary processes through the the pars plana providing pars plana. This is done while looking at visualization of the vitrector the monitor connected to the endoscopic on the left. While doing the system. The IOL is shown above the vitrectomy the monitor endoscopic probe. connected to the endoscopic system, not the microscope, is used to view the procedure.
The endoscope was invaluable in locating and manipulating the lens material. Subsequently, the retina, pars plana, and lens-ciliary body complex could be viewed with the curved endoscope in its entirety. A complete panretinal photoablation was easily done with the ECP settings of 600 mW to 800 mW. After this, attention was turned to the ciliary body. A 180° cyclophotoablation of the ciliary body was performed as well as treatment of the processes to pars plana (Figure 3). An intravitreal injection of dexamethasone was given at the end of the case.
The following day, the patient was pain-free and IOP measured 17 mm Hg and her vision was hand motion. The patient was placed on prednisolone acetate 1% and moxifloxacin. These medications were tapered over 4 weeks. Over the course of the next 3 months, the eye pressure rose to 28 mm Hg and brimonidine 0.1% was started. At 4 months the IOP decreased and the patient’s IOP is 16 mm Hg with no glaucoma medication. The patient feels as though she has some useful vision in this eye. The patient is especially grateful
since the primary open-angle glaucoma has progressed in the other eye and requires a trabeculectomy with mitomycin C, seton or ECP.
Discussion
Neovascular glaucoma is a serious complication of systemic and retinal disease. The IOP can rise rapidly, often resulting in extremely high IOP with irreversible and severe loss of vision. Early panretinal photocoagulation for neovascularization is necessary to ameliorate the devastating sequelae from neovascular glaucoma. Unfortunately, all too often the synechiae between the iris and the lens prevent adequate dilation of the pupil for treatment with panretinal photocoagulation.
Today there is no substitute for panretinal photocoagulation. Transscleral diode laser cyclophotocoagulation is an option for treatment, but it is very destructive to the eye and vision. Usually vision is lost after this type of treatment and hypotony can ensue.
I have found that ECP has tremendous results in patients with vascular glaucoma. A complete panretinal photocoagulation can be performed as well as ablation of the ciliary body at the same time. It avoids the poor visualization issues with a standard vitrectomy and allows for extensive panretinal photocoagulation. ECP in neovascular glaucoma can prevent the need for a glaucoma implant or a trabeculectomy. A 180° ablation of the ciliary body is usually enough to control the IOP without creating hypotony. In vascular glaucoma, the ciliary processes are already damaged and 180° treatment of the ciliary body is usually all that is needed. Other glaucomas usually require at least 270° treatment.
When ablating the ciliary body through the pars plana, it is best to treat all the way to the pars plana because these structures also produce aqueous fluid. Treat the ciliary process until it whitens, shrinks and contracts, but avoid gas bubble formation and audible “popping.” The intensity of the treatment can be adjusted by the distance from the probe to the ciliary body. The closer the probe is to the target, the more intense the treatment. I use 200 mW to 250 mW of laser power. An intravitreal injection of dexamethasone at the end of the case is useful to reduce postoperative inflammation. Dexamethasone is short-lived and usually will not raise the IOP when given in this setting.
In cases of vascular glaucoma, I have not found the need to perform a trabeculectomy or place a glaucoma implant if the ciliary body can be adequately treated with ECP. If the IOP is too high after the first treatment, additional ECP can be performed. A trabeculectomy can be performed as well as placement of a glaucoma implant if necessary. In patients who have conjunctiva that is scarred and vascularized, a trabeculectomy or placement of a glaucoma implant may be difficult. Such cases occur in patients who have had multiple eye surgeries, trauma or chemical burns. Patients with vascular glaucoma usually have such conjunctival tissue. The best choice in many of these cases would be ECP.
References:
Avery RL. Regression of retinal and iris neovascularization after intravitreal
bevacizumab (Avastin) treatment. Retina. 2006;26(3):352-4.
Berke SJ. Endolaser cyclophotocoagulation in glaucoma management.
Techniques Ophthalmol. 2006;4(2):74-81.
Iliev ME, Domig D, Wolf-Schnurrbursch U, Wolf S, Sarra GM. Intravitreal
bevacizumab (Avastin) in the treatment of neovascular glaucoma. Am J Ophthalmol. 2006;142(6):1054-6.
Kawai K. The microendoscope for ciliary process photocoagulation in
neovascular glaucoma. Tokai J Exp Clin Med. 2002;27(1):27-34.
Laatikainen L. A prospective follow-up study of panretinal photocoagulation in
preventing neovascular glaucoma following ischaemic central retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 1983;220(5):236-239.
Lin SC. Endoscopic and transscleral cyclophotocoagulation for the treatment of
refractory glaucoma. J Glaucoma. 2008;17(3):238-247.
Sivak-Callcott JA, O’Day DM, Gass JD, Tsai JC. Evidence-based
recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmol. 2001;108(10):1767-1776.
Tasman W, Magargal LE, Augsburger JJ. Effects of argon laser photocoagulation
on rubeosis iridis and angle neovascularization. Ophthalmol. 1980;87(5):400-402.
Uram M. Ophthalmic laser microendoscope ciliary process ablation in the
management of neovascular glaucoma. Ophthalmol. 1992;99(12):1823-1828.
Wakabayashi T, Oshima Y, Sakaguchi H, et al. Intravitreal bevacizumab to treat
iris neovascularization and neovascular glaucoma secondary to ischemic retinal diseases in 41 consecutive cases. Ophthalmol. 2008;115(9):1571-1580.
Wand M, Dueker DK, Aiello LM, Grant WM. Effects of panretinal
photocoagulation on rubeosis iridis, angle neovascularization, and neovascular glaucoma. Am J Ophthalmol. 1978;86(3):332-339.
Robert F. Haverly, MD, FACS, can be reached at Laser Eye Surgery of Erie, 311
West 24th St., Suite 401, Erie, PA 16502; 814-455-7591; e-mail: [email protected]. Dr. Haverly is a clinical research investigator for Alcon currently and has been a clinical research investigator for Allergan in the past.
The Role of Public-Sector Research in the Discovery of Drugs and Vaccines | Health Poli. Page 1 of 11You are here: Home » Drugs, Devices, and the FDA , Research » The Role of Public-Sector Research in the Discovery of Drugs and Vaccines Research The Role of Public-Sector Research in the Discovery of Drugs and Vaccines NEJM | February 9, 2011 | Topics: Drugs, Devices, and the FDAA
Foglio informativo n. 201/021. Libretto di deposito a risparmio. Libretto nominativo. Informazioni sulla banca. Cassa di Risparmio in Bologna S.p.A. Sede Legale e Amministrativa: Via Farini 22 - 40124 Bologna. Tel.: 800.303.306 (Privati), 800.343.034 (Piccole Imprese), 800.714.714 (Imprese). Sito internet:Iscritta all’Albo delle Banche al n° 5466. Appartenente al gruppo bancario

 Case study: Woman presents with neovascular
Case study: Woman presents with neovascular 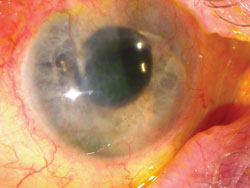 Figure 1. This is the patient’s eye
Figure 1. This is the patient’s eye 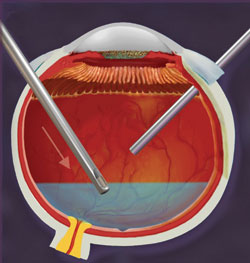
 endoscope was placed through the 19-gauge opening. The Occutome (Alcon) was placed in the superior temporal port and a complete vitrectomy was performed (Figure 2). As the vitreous base was removed, several pieces of white lens material fell onto the macula. The lens remnants were located with the endoscope and removed with the Occutome. At times, the endoscopic probe tip was used to help move and crush the lens material into the Occutome.
Figure 2. The endoscopic
endoscope was placed through the 19-gauge opening. The Occutome (Alcon) was placed in the superior temporal port and a complete vitrectomy was performed (Figure 2). As the vitreous base was removed, several pieces of white lens material fell onto the macula. The lens remnants were located with the endoscope and removed with the Occutome. At times, the endoscopic probe tip was used to help move and crush the lens material into the Occutome.
Figure 2. The endoscopic  Avery RL. Regression of retinal and iris neovascularization after intravitreal
bevacizumab (Avastin) treatment. Retina. 2006;26(3):352-4.
Berke SJ. Endolaser cyclophotocoagulation in glaucoma management.
Techniques Ophthalmol. 2006;4(2):74-81.
Iliev ME, Domig D, Wolf-Schnurrbursch U, Wolf S, Sarra GM. Intravitreal
bevacizumab (Avastin) in the treatment of neovascular glaucoma. Am J Ophthalmol. 2006;142(6):1054-6.
Kawai K. The microendoscope for ciliary process photocoagulation in
neovascular glaucoma. Tokai J Exp Clin Med. 2002;27(1):27-34.
Laatikainen L. A prospective follow-up study of panretinal photocoagulation in
preventing neovascular glaucoma following ischaemic central retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 1983;220(5):236-239.
Lin SC. Endoscopic and transscleral cyclophotocoagulation for the treatment of
refractory glaucoma. J Glaucoma. 2008;17(3):238-247.
Sivak-Callcott JA, O’Day DM, Gass JD, Tsai JC. Evidence-based
recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmol. 2001;108(10):1767-1776.
Tasman W, Magargal LE, Augsburger JJ. Effects of argon laser photocoagulation
on rubeosis iridis and angle neovascularization. Ophthalmol. 1980;87(5):400-402.
Uram M. Ophthalmic laser microendoscope ciliary process ablation in the
management of neovascular glaucoma. Ophthalmol. 1992;99(12):1823-1828.
Wakabayashi T, Oshima Y, Sakaguchi H, et al. Intravitreal bevacizumab to treat
iris neovascularization and neovascular glaucoma secondary to ischemic retinal diseases in 41 consecutive cases. Ophthalmol. 2008;115(9):1571-1580.
Wand M, Dueker DK, Aiello LM, Grant WM. Effects of panretinal
photocoagulation on rubeosis iridis, angle neovascularization, and neovascular glaucoma. Am J Ophthalmol. 1978;86(3):332-339.
Robert F. Haverly, MD, FACS, can be reached at Laser Eye Surgery of Erie, 311
West 24th St., Suite 401, Erie, PA 16502; 814-455-7591; e-mail:
Avery RL. Regression of retinal and iris neovascularization after intravitreal
bevacizumab (Avastin) treatment. Retina. 2006;26(3):352-4.
Berke SJ. Endolaser cyclophotocoagulation in glaucoma management.
Techniques Ophthalmol. 2006;4(2):74-81.
Iliev ME, Domig D, Wolf-Schnurrbursch U, Wolf S, Sarra GM. Intravitreal
bevacizumab (Avastin) in the treatment of neovascular glaucoma. Am J Ophthalmol. 2006;142(6):1054-6.
Kawai K. The microendoscope for ciliary process photocoagulation in
neovascular glaucoma. Tokai J Exp Clin Med. 2002;27(1):27-34.
Laatikainen L. A prospective follow-up study of panretinal photocoagulation in
preventing neovascular glaucoma following ischaemic central retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 1983;220(5):236-239.
Lin SC. Endoscopic and transscleral cyclophotocoagulation for the treatment of
refractory glaucoma. J Glaucoma. 2008;17(3):238-247.
Sivak-Callcott JA, O’Day DM, Gass JD, Tsai JC. Evidence-based
recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmol. 2001;108(10):1767-1776.
Tasman W, Magargal LE, Augsburger JJ. Effects of argon laser photocoagulation
on rubeosis iridis and angle neovascularization. Ophthalmol. 1980;87(5):400-402.
Uram M. Ophthalmic laser microendoscope ciliary process ablation in the
management of neovascular glaucoma. Ophthalmol. 1992;99(12):1823-1828.
Wakabayashi T, Oshima Y, Sakaguchi H, et al. Intravitreal bevacizumab to treat
iris neovascularization and neovascular glaucoma secondary to ischemic retinal diseases in 41 consecutive cases. Ophthalmol. 2008;115(9):1571-1580.
Wand M, Dueker DK, Aiello LM, Grant WM. Effects of panretinal
photocoagulation on rubeosis iridis, angle neovascularization, and neovascular glaucoma. Am J Ophthalmol. 1978;86(3):332-339.
Robert F. Haverly, MD, FACS, can be reached at Laser Eye Surgery of Erie, 311
West 24th St., Suite 401, Erie, PA 16502; 814-455-7591; e-mail: