Cetirizine and pseudoephedrine retard, givenalone or in combination, in patients with seasonalallergic rhinitis*
M. Grosclaude1, K. Mees2, M.E. Pinelli3, M. Lucas3, H. Van de Venne3
Centre Claude Bernard, Guilherand-Granges, France
HNO-Klinik Grosshadern, München, Germany
UCB S.A. Pharma Sector, Braine-l’Alleud, Belgium
We compared the efficacy and safety of cetirizine (5 mg), pseudoephedrine retard (120 mg),and the combination of cetirizine (5 mg) with pseudoephedrine retard (120 mg), each giventwice daily for two weeks to subjects with pollen-associated allergic rhinitis. The study wasmulticentre and of randomized, double-blind, parallel-group design. Five rhinitis symptomswere rated according to severity on a scale of 0-3, daily by patients and at each clinic visit byinvestigators. A total of 687 patients, aged 9-66 years (mean: 32 years) was randomised totreatment (cetirizine: 231; pseudoephedrine: 226; combination: 230). On entry, the threegroups were comparable in relevant respects. The primary outcome measure was based on thefive symptoms assessed by the patients over the 2-week treatment period. The combination wasmore effective, providing at least 20% more “comfortable days” (symptoms absent or at mostmild) than cetirizine or pseudoephedrine given alone (median values: 53.3%, 30.8%, and33.3%, respectively; p<0.001). For nasal obstruction, the combination (mean score: 1.19) wasmore effective than cetirizine (mean score: 1.43; p=0.0005), but there was little differencebetween the combination and pseudoephedrine (mean score: 1.22; not significant). Sneezing,rhinorrhoea, nasal and ocular pruritus were better controlled by combination (mean 4-symp-tom score: 0.77) than by pseudoephedrine alone (mean 4-symptom score: 1.12; p<0.001) andalso better than by cetirizine alone (mean 4-symptom score: 0.93; p<0.001). No unexpectedadverse reactions were observed. A combination of cetirizine and pseudoephedrine retard iswell tolerated and superior to each given alone for moderate to severe allergic seasonal rhini-tis, especially when nasal obstruction is a predominant symptom.Keywords: cetirizine, pseudoephedrine, seasonal rhinitis, allergic rhinitis
allergic rhinitis (Falliers et al., 1991; Mansmann et al., 1992; Masi
The treatment of symptoms of seasonal allergic rhinoconjuncti-
et al., 1993; Jobst et al., 1994). Cetirizine is normally taken as a
vitis often requires the use of an antihistamine to control symp-
single daily dose of 10 mg, but a dose of 5 mg twice daily has been
toms primarily mediated by histamine, such as sneezing,
shown to be as effective (Wassemlan et al., 1991).
rhinorrhoea, nasal and ocular pruritus, together with a deconge-
Relief of nasal congestion by pseudoephedrine, taken orally, is
stant to improve nasal congestion when it is a prominent sympt-
well documented, both when it is taken alone (Roth et al., 1977;
Hamilton et al., 1982) and in combination with an H -antagonist
Each new fixed-combination product must be shown to be more
agent (Backhouse et al., 1990; Bronsky et al., 1995; Bertrand et
effective than its components given as sole therapy. More precise-
al., 1996; Dockhorn et al., 1996). The maximal daily dose of
ly, the combination must at least provide better control of nasal
pseudoephedrine is 240 mg, in adults and children 12 years and
obstruction than the antihistamine alone, and be superior to pseu-
over, even in over-the-counter products in the United States
doephedrine alone in treating the other symptoms of rhinitis.
Cetirizine is a potent, selective H -antagonist of established effica-
The present study examined the efficacy and safety of cetirizine
cy and good tolerability in the treatment of seasonal and perennial
(5 mg) and pseudoephedrine retard (120 mg), each given twice
* Received for publication August 1, 1996; accepted November 15, 1996
daily, with a combination formulation of cetirizine and pseu-
allergic rhinitis; (2) escalating doses of desensitization therapy;
doephedrine in subjects with pollen-associated allergic rhinitis.
and (3) participation in another drug trial during the preceding
A placebo group was not considered to be needed as the trial
three months. Pregnant or lactating women were not included.
aimed at evaluating the superiority of the combination over
Patients who had taken any of the following medications within
the periods specified were excluded from entry: (1) astemizole
(6 weeks); (2) systemic corticosteroids, ketotifen or MAO inhi-
bitors (2 weeks); (3) topical corticosteroids or sedatives (1
week); or (4) nasal decongestants, antihistamines other than
The study was multicentre and of double-blind design. Patients
astemizole and ketotifen, and nasal or ocular cromoglycate (2
were allocated, in blocks of three, stratified by centre, from a
days). Concomitant use of any of these agents during the trial
computer-generated randomisation list, to one of three treat-
led to withdrawal, as well as other protocol violations, ineffica-
ments: 5 mg cetirizine alone; 120 mg pseudoephedrine retard
cy, adverse events or personal reasons.
alone; and the same doses of both agents in combination.
Treatment with each regimen was given twice daily for two
weeks to subjects with pollen-associated allergic rhinitis. A total
Patients were randomized to one of the following treatment
of 43 centres participated in the study, 30 in France and 13 in
regimens: (1) cetirizine (5 mg) and pseudoephedrine retard
Germany. The study was performed between March and
placebo; (2) pseudoephedrine retard (120 mg) and cetirizine
September 1992, when pollen counts were high (data not
placebo; and (3) cetirizine (5 mg) and pseudoephedrine (120
mg). All medications were in capsules of identical appearance
The study was conducted in accordance with the amended
and taken twice daily with meals. No rescue medication was
Declaration of Helsinki (Tokyo, 1991) and the European
Community Guidelines on Good Clinical Practice (1990).
Medications prohibited during the study were corticosteroids
Patients, their parents or guardians gave their written informed
(except inhaled steroids in a dose ≤400 µg/day), sedatives, topic-
consent and the study protocol was approved by relevant Ethics
al nasal and ocular medications, appetite suppressants, amphe-
tamine CNS stimulants, cromones other than by inhalation,
The study required three visits of the patient: on entry, review
after one week, and a final visit after two weeks’ treatment. Male
Medications for the treatment of asthma (theophylline, ß2-sym-
and female out-patients (aged 12-65 years) with a documented
pathomimetic drugs, inhaled cromoglycate, nedocromil, inha-
history of pollen-associated allergic rhinitis for at least one year
led corticosteroids in a dose ≤400 µg/day) and non-steroidal
and skin or RAST tests positive to seasonal allergens were
topical agents for atopic dermatitis could be taken, provided that
admitted to the study. Women of childbearing potential had to
be using a medically acknowledged method of contraception
and a negative pregnancy test was required prior to enrollment.
On entry, all patients presented with nasal obstruction together
On entry to the study, the findings from history and physical
with at least two of the following symptoms of rhinitis: snee-
examination were recorded. On entry, at review one week later
zing, rhinorrhoea, nasal pruritus, or ocular pruritus. Symptoms
and at the final visit, investigators evaluated the following symp-
were scored on a 4-point scale: “0”: absent; “1”: mild (present
toms of allergic rhinitis: nasal obstruction, sneezing, rhinor-
but not disturbing); “2”: moderate (disturbing but not hampe-
rhoea, nasal pruritus, and ocular pruritus - using the 4-point
ring daily activities or sleep); and “3”: severe (hampering daily
activities and/or sleep). Nasal obstruction on the day of admis-
Patients evaluated the same symptoms (sneezing, runny nose,
sion was at least moderate in degree (score 2) and the total score
blocked nose, itchy nose, and itchy eyes) each day using the
for the five symptoms was at least 8 (of a possible 15), indicating
same 4-point scale and the results, entered in the patients’ dia-
rhinitis of moderate to severe degree.
ries, constituted the primary efficacy variables. At the final
Patients to whom any of the following criteria applied were not
assessment, the investigator made a global evaluation of the
eligible for inclusion: (1) asthma, requiring either a change in
effect of treatment using the following 5-point scale: “0”: worse;
treatment, or systemic or inhaled corticosteroids in a dose more
“1”: no change; “2”: slight improvement; “3”: marked improve-
than 400 µg/day; (2) atopic dermatitis or urticaria requiring anti-
histamines or systemic or topical corticosteroids; (3) an upper
Heart rate and blood pressure were checked at each visit; all
respiratory tract infection present on the day of admission; (4)
adverse events together with outcome, severity, duration and pos-
obstructive nasal polyps or significant septal deviation; (5) rele-
sible causal relationship with the study drugs were recorded and
vant renal, hepatic or cardiovascular disease requiring treat-
classified according to the COSTART dictionary (DHHS, 1989).
ment; (6) hypertension; (7) hyperthyroidism; (8) diabetes; (9)
Blood was taken for routine laboratory safety tests (full blood
glaucoma; (10) prostatic hypertrophy; (11) urinary retention;
count, haematocrit, SGOT, SGPT, total serum bilirubin, blood
(12) hypersensivity to cetirizine or pseudoephedrine; and (13)
urea, and plasma creatinine) at the first and last visits.
an infection requiring antibiotic treatment. Other reasons for
Returned tablets were counted to determine compliance with
exclusion were: (1) clinically relevant abnormalities unrelated to
study medication, which was required to be between 80 and 120%. Cetirizine/pseudoephedrine in seasonal rhinitis
Table 1. Patients enrolled and completing the study: Reasons for with-
Patients’ evaluations: The primary efficacy measure was based
on the scores for the five symptoms, as assessed by the patients,
over the total treatment period. The highest score of any one of
the five symptoms, i.e. the score of the most severe symptom,
was calculated each day for each patient, and this was called the
“maximal symptom score.” The percentage of days with a maxi-
mal score of 0 or 1, called “comfortable” days, was computed
from the second day of treatment to the day before the last visit.
This primary outcome measure was selected since in our opin-
ion it provides the most clinically relevant global measure of
effective treatment of rhinitis, i.e. when symptoms do not dis-
The Kruskal-Wallis test was used to compare the distribution of
this variable between study groups, with a significance level of
5%. Comparisons of each of cetirizine and pseudoephedrine
with the combination were performed using the Wilcoxon rank
sum test, with a significance level of 3%.
Secondary efficacy variables were the mean 5-symptom score,
Table 2. Patients’ characteristics at baseline.
the mean 4-symptom score (excluding nasal congestion) and
individual mean symptom scores, over the whole treatment
period. Global comparisons were performed on the variable
using one-way analysis of variance, and two-by-two compari-
sons were performed using Student’s t test. Investigators’ evaluations: The severity of rhinitis at each visit
was assessed by selecting the highest score of the five symp-
toms. They were compared at each visit using the Cochran-
Mantel-Haenszel (CMH) test stratified according to baseline
(highest score at visit 1). Investigators’ global evaluations at the
end of the study were also compared using the CMH test. Safety: The number of patients in each treatment group with
none, one, two, three or more adverse events was compared
positive allergy tests* (% patients):
Data from all patients receiving treatment were analysed on an
intention-to-treat basis. Analyses were performed using SAS
software, Versions 6.07 and 6.09 for VMS.
Of 687 patients with pollen-associated allergic rhinitis random-
ized in the study by 43 investigators, 231 were randomized to
severity of rhinitis (mean scores from patient diaries):
cetirizine, 226 to pseudoephedrine and 230 to combination
treatment with cetirizine and pseudoephedrine (Table 1). Three
patients in each group did not return their daily record cards. A
total of 616 patients (89.7%) evenly distributed between the
three treatment groups completed the study. The reasons for
withdrawal in 71 patients were lack of efficacy (30 patients);
adverse events (22 patients); and other reasons unrelated to
study drugs, mostly protocol deviations (19 patients; Table 1).
*: not all allergens were tested in every patient; **: excluding blocked
The three groups were closely comparable in baseline characte-
ristics: age, sex, body weight, allergies, duration of rhinitis, and
severity of symptoms (Table 2). Since all patients had to have at
Average compliance with treatment was estimated at 97-99%. The
least one symptom of moderate severity to be eligible, there
numbers and types of concomitant therapies prescribed during the
were no “comfortable days” at baseline. As requested, nasal
study were also similar in the various groups and consisted chiefly
obstruction was of moderate to severe degree and a prominent
of anti-asthmatics (28-32 in each group), topical nasal preparations
symptom with mean scores of 2.2-2.3 across the three groups
(13-15 in each group), ophthalmic preparations (9-15 in each group)
and maintenance desensitization (11-13 in each group). Five symptoms: At baseline, all patients had moderate to severe
symptoms and mean scores were comparable (Table 2). During
the 2-week treatment period, the proportion of “comfortable”
days (symptoms absent or mild at the most) was significantly
(p< 0.001) greater with the combination than with either cetiri-
zine or pseudoephedrine alone; the median values were 53.3%,
30.8% and 33.3%, respectively, and the mean values 50.5%,
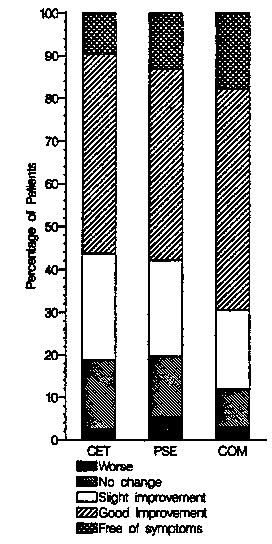
Figure 3. Global evaluation of treatment by investigators (CET: cetiri-
Figure 1. Percentage of “comfortable” days (no or only mild symp-
zine; PSE: pseudoephedrine; COM: combination).
toms); •: median; ×: mean; bars represent the first and third quartile;CET: cetirizine; PSE: pseudoephedrine; COM: combination.
39.8% and 37.2%, respectively (Figure 1). The same conclusion
Table 3. Mean scores over total treatment period for five symptoms, four
was reached for the mean 5-symptom scores which were 0.85,
symptoms and individual symptoms (daily record cards).
1.03 and 1.14, respectively (Table 3). Four symptoms: The mean score of the four symptoms (sneez-
ing, rhinorrhoea, nasal and ocular pruritus) over the total treat-
ment period was significantly (p<0.001) lower for the combina-
tion (0.77) than for cetirizine (0.93) or pseudoephedrine (1.12)
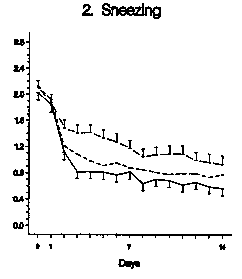
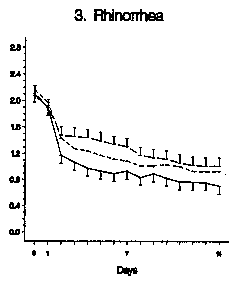
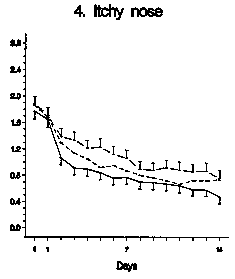
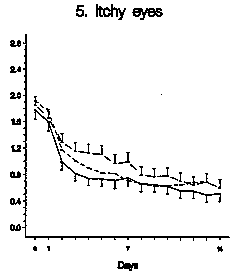
Individual symptoms: Baseline scores for all symptoms were
similar in the three groups (Table 2). The pattern and time-
course of improvement in mean scores is shown in Figure 2
(graphs 1-5). Improvement was significantly (p≤0.01) greaterwith combination treatment than with cetirizine for all symp-
toms (except itchy eyes) and greater than pseudoephedrine alo-
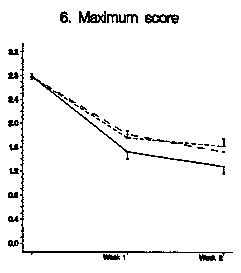
ne for all symptoms, except nasal congestion (Table 3). Maximal symptom scores: The mean maximal score of the five
symptoms as assessed by investigators was calculated for each
visit. Baseline values were similar in the three groups (2.77-
comparisons versus combination: **0.001<p≤0.01;***p < 0.001
2.78). Investigators judged combination therapy (mean maxi-
Cetirizine/pseudoephedrine in seasonal rhinitis
Figure 2. Graphs 1-5: Mean individual symptom scores rated daily by patients. Graph 6: Mean maximal symptom scores rated by investigators at thevisits (bars represent two standard errors).
mum score: 1.53) to be significantly more effective than either
mouth (pseudoephedrine 4.4%; combination 7.4%). Minor labo-
cetirizine or pseudoephedrine (mean maximum score: 1.76 and
ratory test abnormalities in 7 patients were not considered
1.82, respectively; p<0.01) as sole therapy after the first week
clinically relevant. Mean heart rate increased by 2.2 and 3.2
and also after the second week (combination: 1.29; cetirizine:
beats/min, between the first and the last visit, respectively in the
1.63, [p<0.001]; pseudoephedrine: 1.53 [p=0.031]). The pattern
pseudoephedrine and combination groups.
of response for the mean maximal score of the five symptoms is
apparent in Figure 2 (graph 6). Nasal obstruction scores with
combination treatment were significantly lower than after cetiri-
These results in a large group of patients with pollen-associated
zine (p<0.001) but not pseudoephedrine, after both one and two
allergic rhinitis of moderate to severe degree show that combi-
ned treatment with cetirizine and pseudoephedrine provides
Global evaluation of treatment: Analysis of investigators’ global
greater symptom relief than either agent alone. The combina-
evaluations of treatment also confirmed that combination
tion led to more improvement than pseudoephedrine alone in
therapy was significantly more effective than either cetirizine
“histamine-induced” symptoms of sneezing, rhinorrhoea, nasal
(p=0.001) or pseudoephedrine (p=0.007) taken alone (Figure 3).
and ocular pruritus. Compared with cetirizine, the combination
Good to excellent results were reported by 69% of the patients
was, as anticipated, more effective in relieving nasal congestion,
in the combination group, in 56% of the patients in the cetirizi-
but also the other three nasal symptoms (sneezing, rhinorrhoea
ne group, and in 58% in the pseudoephedrine group.
and nasal pruritus). A likely explanation for this finding is a
“carry-over” effect due to the good relief from the nasal conges-
tion on the evaluation of the other nasal symptoms.
Adverse events (Table 4), whether or not considered drug-
We defined the primary criterion of efficacy as the overall effect
related, were reported by 54 patients (23.4%) taking cetirizine,
of treatment over the 2-week study period and expressed this as
68 patients (30.1%) with pseudoephedrine, and 68 patients
the percentage of “comfortable days”, i.e. days when patients
(29.6%) with combination treatment (not significant). There
were without symptoms, either moderate or severe in intensity.
were no serious adverse events. Adverse events were infre-
We have previously explained why we believe this analysis is to
quently considered severe and led to withdrawal from the study
be preferred (Masi et al., 1993; Jobst et al., 1994) to a more con-
in 6 patients (2.6%) on cetirizine, 7 patients (3.1%) on pseudo-
ventional analysis of mean (or total) symptom scores. This ana-
ephedrine, and 9 patients (3.9%) on combination treatment.
lysis is more demanding since it is driven by the least responsive
symptom, but in the present instance it helped in separating the
effects of the three treatments. However, we also analysed the
mean scores to confirm our findings and again found the com-
bination to be more effective than either of its components.
The results of investigators’ evaluations, made at review visits
after one and two weeks, also confirmed the greater efficacy of
combination treatment. For this analysis we used again the
maximal scores, i.e. the scores of the most severe symptom, to
characterize disease severity. Global evaluations by investiga-
tors at the end of the study also favoured combination treat-
The incidence of adverse events was in line with the known
safety profiles of the agents and there were no unexpected or
serious adverse events. The incidence of severe adverse events
was twice as high with combination treatment compared to ceti-
number of patients (%) with most frequent adverse events:
rizine alone. This is the price which must be paid for increased
efficacy, as suggested by the drop-out rates: more withdrawals
because of adverse events with combination treatment and, by
contrast, more due to lack of efficiency with the single agents.
The results of this trial are consistent with those of comparable
combination products (Backhouse et al., 1990; Bronsky et al.,
1995; Dockhorn et al., 1996) and of a previous study in which
*possibly drug-related adverse events: cetirizine: 2; pseudoephedrine:
cetirizine and pseudo-ephedrine alone were compared with the
combination in patients with perennial allergic rhinitis
(Bertrand et al., 1996). We conclude that a combination of ceti-
Adverse events reported most frequently were somnolence
rizine (5 mg) and pseudoephedrine retard (120 mg), both given
(6.1%) and headache (4.3%) with cetirizine, and in those on
twice daily over a 2-week period, is a well tolerated and effective
pseudoephedrine and combination treatment, headache (pseu-
treatment for the symptoms of seasonal allergic rhinitis, par-
doephedrine 7.1%; combination 3.9%), sleep disorders, mostlyinsomnia (pseudoephedrine 11.1%; combination 6.9%) and dry
ticularly when nasal congestion is a prominent symptom. Cetirizine/pseudoephedrine in seasonal rhinitis
7. Hamilton LH, Chobanian SL, Cato A, Perkins JG (1982) A study of
The authors thank all participating investigators in France and
sustained action pseudoephedrine in allergic rhinitis. Ann Allergy48: 87-92.
Germany. They are indebted to J.L. Marchal for supplementary
8. Jobst S, Van den Wijngaart W, Schubert A, Van de Venne H (1994)
statistical analyses, and to C. Arendt for the medical monitoring
Assessment of the efficacy and safety of three dose levels of cetiri-
zine given once daily in children with perennial allergic rhinitis. Allergy 49: 598-604.
9. Mansmann Jr. HC, Altman RA, Berman BA, Buchrnan E,
Dockhorn RJ, Leese PT, Love SJ, Middleton Jr E (1992) Efficacy
1. Backhouse Cl, Rosenberg RM, Fidler C (1990) Treatment of aller-
and safety of cetirizine therapy in perennial allergic rhinitis. Ann
gic rhinitis: A comparison of a combination tablet of terfenadine
and pseudoephedrine with individual ingredients. Br J Clin Pract
10. Masi M, Candiani R, Van de Venne H (1993) A placebo-controlled
trial of cetirizine in seasonal allergic rhinoconjunctivitis in children
2. Bertrand B, Jamart J, Marchal JL, Arendt C (1996) Cetirizine and
aged 6 to 12 years. Pediatr Allergy Immunol 4 (Suppl 4): 47-52.
pseudoephedrine retard alone and in combination in the treatment
11. Roth RP, Cantekin EI, Bluestone CD, Welch RM, Cho YW (1977)
of perennial allergic rhinitis: A double-blind multicentre study.
Nasal decongestant activity of pseudoephedrine. Ann Otol 86: 235-
3. Bronsky E, Boggs P, Findlay S, Gawchik S, Georgitis J, Mansmann
12. USCFR (1996) Labeling of Nasal Decongestant Drug Products.
H, Sholler L, Wolfe J, Meltzer E, Morris R, Munk Z, Paull B,
Code of Federal Regulations 21/CFR341.80, p. 258.
Pleskow W, Ratner P, Danzig M, Harrison J, Lorber R (1995)
13. Wassemlan SI, Broide DH, Marquardt DL (1991) Cetirizine thera-
Comparative efficacy and safety of a once daily loratadine/pseu-
py for seasonal allergic rhinitis: Alternative dosage schedules. Clin
doephedrine combination versus its components alone and placebo
in the management of seasonal allergic rhinitis. J Allergy ClinImmunol 96: 139-147.
4. DHHS (1989) “COSTART” Coding Symbols for Thesaurus of
Adverse Reaction Terms. Department of Health and Human
Services/Food and Drug Administration, Washington, USA.
5. Dockhorn RJ, Williams BO, Sanders RL (1996) Efficacy of acrivas-
tine with pseudoephedrine in treatment of allergic rhinitis due to
ragweed. Ann Allergy Asthma Immunol 76: 204-208.
6. Falliers CJ, Brandon ML, Buchman E, Connell JT, Dockhorn R,
Leese PT, Miller J, Wasserman Sl, Zeterberg JM, Altman R, Love S,
Samuels LL (1991) Double-blind comparison of cetirizine and place-bo in the treatment of seasonal rhinitis. Ann Allergy 66: 257-262.
“HEARTLESS EXPLOITATION OF THE POOR AND SUFFERING”? Note: Center Discussion Papers are preliminary materials circulated to stimulate Abstract The decision to require that countries grant product patents for pharmaceutical innovations as a condition of membership in the World Trade Organization was verycontentious. Almost fifty developing countries were not granting patent monopolies for
Office of the Contractor-General Public Body Contract Awards (J$275,001 to J$10,000,000 in Value) Quarterly Contract Awards (QCA) Report QCA Report submitted to the Contractor General pursuant to Section 4(2)(a) and 4(3) of the Contractor-General Act COMPLETE ONLY AFTER READING INSTRUCTIONS IN APPENDIX B . SELECT APPLICABLE PRINT RANGE BEFORE PRINTING SECTION 1 (1) Name of Reportin
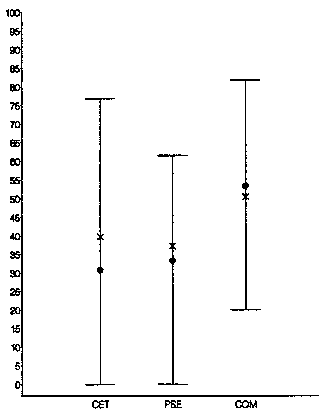
 Five symptoms: At baseline, all patients had moderate to severe
symptoms and mean scores were comparable (Table 2). During
the 2-week treatment period, the proportion of “comfortable”
days (symptoms absent or mild at the most) was significantly
(p< 0.001) greater with the combination than with either cetiri-
zine or pseudoephedrine alone; the median values were 53.3%,
30.8% and 33.3%, respectively, and the mean values 50.5%,
Figure 3. Global evaluation of treatment by investigators (CET: cetiri-
Figure 1. Percentage of “comfortable” days (no or only mild symp-
zine; PSE: pseudoephedrine; COM: combination).
Five symptoms: At baseline, all patients had moderate to severe
symptoms and mean scores were comparable (Table 2). During
the 2-week treatment period, the proportion of “comfortable”
days (symptoms absent or mild at the most) was significantly
(p< 0.001) greater with the combination than with either cetiri-
zine or pseudoephedrine alone; the median values were 53.3%,
30.8% and 33.3%, respectively, and the mean values 50.5%,
Figure 3. Global evaluation of treatment by investigators (CET: cetiri-
Figure 1. Percentage of “comfortable” days (no or only mild symp-
zine; PSE: pseudoephedrine; COM: combination).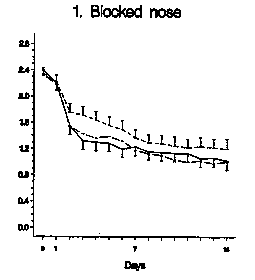
 Cetirizine/pseudoephedrine in seasonal rhinitis
Figure 2. Graphs 1-5: Mean individual symptom scores rated daily by patients. Graph 6: Mean maximal symptom scores rated by investigators at thevisits (bars represent two standard errors).
Cetirizine/pseudoephedrine in seasonal rhinitis
Figure 2. Graphs 1-5: Mean individual symptom scores rated daily by patients. Graph 6: Mean maximal symptom scores rated by investigators at thevisits (bars represent two standard errors).