Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Asd intervention vienna oct 07.ppt
The Autism Spectrum Disorders: Interventions Vienna, October 2007 Definitions
Autism = Autism Spectrum Disorders (ASM) =Pervasive Developmental Disorders (PDD)
v The ASM encompass the entire range of severityv The ASM diagnosis applies irrespective of etiologiesv Dimensional, not dichotomous Dx ’ fuzzy margins,
DSM IV PDD
PDD = pervasive developmental disorder,
1. Autistic disorder2. Asperger disorder3. PDD-NOS (PDD not otherwise specified)
4. Disintegrative disorder5. (Rett disorder)
Etiologies of Autism
§ In ~ 80-90% of cases, etiology unknown but
genetically (and environmentally?) influenced
§ Diagnosable causes multiple but each exceedingly
Potential targets of intervention
v Not available because many putative etiologies
v Multiple ’ even if known, no one Rx applies to all
v Main neuropathologic evidence: prenatal processv Pharmacology: targets putative monoamines, etc.
v Education, i.e., influence brain development/
Needs to be addressed
v Core deficits: educational/behavioral intervention
v Associated symptoms (e.g., epilepsy, apraxia,
ADHD, etc.) that need medical or other Rx
v Education about autism and how to deal with it
v Emotional support for all family members
Problems with the evidence
studies of the effectiveness of behavioral or medical interventions
comparing the effectiveness of different treatment approaches
children, ill-defined selection criteria, short-term studies
Symptoms to be remediated
§ Troublesome social behaviors, especially
aggressivity, joint inattention, tantrums
§ Troublesome stereotypies & rigidity
v functional MRI in amputees, blindness, deafness
§ But efficacy of intervention is constrained
by the severity of the underlying brain dysfunction
addresses some troublesome symptoms, not core deficits
Age at intervention
§ The brain is most plastic while brain
§ The earlier targeted education starts,
crucial (even though controlled studies not available to show this in autism)
Characteristics of early intervention
§ Must be individualized to each child’s
Educational management
§ No cure! – the goal is optimal functional outcome - within the constraints of individual brain biology! ’ less severely affected children do better…
§ Child needs to be taught specific social & other skills that other children “pick up” on their own
§ Parents need training in behavior management § Address needs of all family members! § Discourage unproven therapies Needs of other family
§ All need to be aware of goals/strategies of
§ All need to learn what autism is & is not
v Personal support, on-going individual helpv Training in management strategiesv Respite & practical assistancev Opportunity to fulfill their own needs
v Must not to be sacrificed to autistic sibv Need to learn to be tolerant helpers and advocates
Treatments of unproven specificity / efficacy
Chelation of heavy metals (mercury, lead)
Sensory integration, vestibular stimulation
Anticonvulsants in the absence of clinical epilepsy? OK for their psychotropic effects
Approaches to behavioral remediation
§ All require preliminary and on-going functional behavioral
§ Developmental Individual Differences (Floor Time) (Greenspan) (one
on one - encourages interaction and progress through developmental milestones)
§ Individual operant conditioning: Applied Behavior Analysis - ABA
(Loovas), pivotal response training (Koegel) etc. - effective to develop compliance, but not panacea (one on one, no peers, may not generalize)
§ Structured teaching: Treatment & Education of Autistic and Related
Communication Handicapped Children (TEACCH) (Schopler) (addresses needs of family & child)
§ Integrated education: normal peers (± individual coach): provide
role models, supplemented with individual training
§ Mixed models (including parents in the classroom)
Remediation of social problems
§ Bring child under adult control (compliance)§ Train joint attention, sitting§ Teach/pactice social interactions (with
§ Teach how to read social cues§ Teach how to react to frustration§ Teach that temper tantrums are no longer
Remediation of social problems
§ Provide varied & graded opportunities to
v interact with small, then larger, groups of peers
(e.g., well supervised nursery school, play dates,
v participate in community activities (school,
In schoolage children
§ Ongoing social skills training in dyadic or
triadic groups of specific & realistic interactions, with feedback and practice between training sessions
§ Use of visual organizers to provide visual
frameworks that demonstrate paths of interactions
§ Training teachers & parents to do the
Communication deficits
§ Focus on meaningful communication through any
channel (pragmatics are universally and persistently impaired)
§ Operant conditioning often useful to get language
started, but inadequate to train spontaneous/ conversational language use
§ Visual language (pictures, Sign): does not retard/ inhibit
Rigidity
§ Written/drawn schedules to minimize surprises
§ Announce changes in advance
§ Gradually practice flexibility – deliberate schedule deviances Stereotypies
§ Ignore stereotypies that are not too frequent unless they preclude more meaningful activities
§ Operant conditioning to minimize troublesome stereotypies
§ Medication? Atypical sensory responses
§ Effectiveness of intervention is limited
§ Ignore those that are not too troublesome
§ Choose those stimuli to which to attempt desensitization
§ Try to avoid the most troublesome stimuli
§ No effective drug known Self-injury
§ Extremely difficult to treat § Analyze circumstances of its occurrence to avoid them
§ No truly effective medication, including naltrexone
§ Anafranil, SSRIs? – may be useful for obsessive/compulsive picking at sores Sleep disorders
§ Goal: consolidate night sleep§ Avoid daytime naps§ Have regular sleep time § Institute going to bed routine, resist
(chloral hydrate, clonidine, guanfacin, welbutrin?)
Pharmacotherapy: role and limitations
§ Adjunctive to behavioral interventions
§ Questionable use of multiple medications
Attention deficit
§ Poor joint attention or real ADD? § Use same behavioral approaches as for ADD. May/may not need medication
§ Try stimulants: help some children, and effect ~ immediate and short-lived (methylphenidate, atomoxetine?)
§ Other drugs: clonidine, guanfacine, paroxetine? § Avoid risperidone unless there are other troublesome symptoms like aggressivity Aggression, irritability
§ Dopamine blockers (haloperidol etc.) effective but
major side-effects (sedation, dystonic & tardivedyskinesias, weight gain, etc.)
§ Atypical neuroleptics, specific serotonin reuptake
inhibitors - SSRIs (risperidone, paroxetine, fluvoxamine, fluoxetine, etc)
§ Anxiolytics (SSRIs, propranolol, benzodiazepines)§ Antidepressants (clomipramine, desipramine)§ Anticonvulsants as mood stabilizers (valproate,
Autism: Epilepsy
Ø Cumulative risk: 30% by adulthoodØ Onset peaks: toddler/preschool,
Ø Linked to severity of MR and other signs
Risk Factors for Seizures in Children with Autism Epilepsy in children without severe MR classified by language subtype Epilepsy
§ Clinical seizures are treated to achieve control as they would in any child
§ Choice of medication: avoid sedative or other behavioral side-effects
§ No evidence to date that medication is effective for subclinical epilepsy/EEG epileptiform activity, even in the face of language/autistic regression or ESES (dissenting opinion in selected cases: Deonna/Roulet-Perez, 2005) Autistic Regression
Ø Regression of language, sociability, playØ Mean age: 21 monthsØ Reported by 1/3 of parentsØ Improvement but not full recovery after a
Ø Trigger?Ø Role of subclinical epilepsy?
Treatment of autistic regression
anticonvulsants effective for subclinical epileptiform activity, even in the face of language/autistic regression!
§ Only anecdotal reports of effectiveness
AUTISM: PROGNOSIS
v Symptoms change with agev Improve with early intensive educationv Prognosis unreliable in early childhoodv So do not “hang crepe” too early
Autism: Prognosis
v Prognosis variable, by no means hopeless, unreliable in very young
v Depends in part on the adequacy of family’s and
v Supplement auditory by visual inputsv Provide a structured predictable environmentv Train social skills throughout childhood
ElderCare Online’s Learning Resource GuideThe following Glossary of Elder Care Terminology covers medical terms, medicalconditions, health care services and programs, gerontology terms and Medicare andMedicaid terms. While some medical conditions or treatments may be mentionedhere, this guide does not endorse any treatments and it is not a comprehensive text. You should consult your medical,
SECOORA SUMMER PHYSICAL SCIENCE WORKSHOP PRIOR TO THE WORKSHOP WHAT YOU NEED TO KNOW.DAY ONE.MONDAY Meeting Place for Monday: (See attached map for directions.) Meeting Time for Monday: What to Wear: Comfortable clothing (shorts, tennis shoes, etc.) What to Bring on Monday: • Sun Protection (hat, sun visor, sunglasses, sun screen) • Water bottle. • Lunch, snacks, and any
 Risk Factors for Seizures
Risk Factors for Seizures 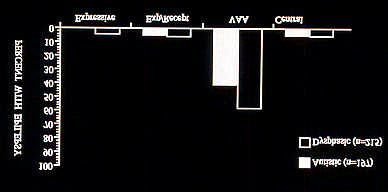 Epilepsy in children without severe
Epilepsy in children without severe