Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
A case of a patient with sunct syndrome treated with jannetta procedure
A case of a patient with SUNCT syndrome treated with
L Gardella, A Viruega, H Rojas & J NagelSanatorio Parque, Cordoba, Rosario, Santa Fe, Argentina
Gardella L, Sanatorio Parque, Cordoba 2324, Rosario (CP 2000), Santa Fe, Argentina. Received 12 September 2000, accepted 18 June 2001
wind, lateral head movements to the right and rapid eye
movements also triggered the pain.After the painful
SUNCT syndrome is a rare disorder.Sjaastad (1) ®rst
episodes she suffered from hyperesthesia in the affected
described this syndrome in 1978.The patient suffers
area and the skin of the ipsilateral frontal region looked
short-lasting, unilateral crisis of a neuralgic-type pain
rough and irregular like `sandpaper'.Neurological
of a severe intensity, centred in the orbital/periorbital
examination, except for the above description, was
area.This pain is accompanied by conjuctival injection,
always normal.The previous clinical history and the
CT scan were unremarkable.Indomethacin, amitripty-
This syndrome has some similarities with cluster
line, ergotamine and verapamil treatments were not
headache (17) and ®rst-division trigeminal neuralgia.
helpful.The later use of prednisolone (60 mg daily for
The treatment is carbamacepine, amitrptyline, pred-
6 days and then 20 mg daily for 10 days) and carbama-
nisolone, indomethacin, verapamil, ergotamine, with
cepine (800 mg per day for 11 weeks) brought bene®t
unlikely and uncertain results (18).Very few cases
by reducing the painful crises to one or two a day, but
Because of these negative therapeutic results, we
considered surgical methods (17, 20, 21).
A 48-year-old woman consulted a physician in April
1997 due to a painful condition in the right orbitofrontal
area.She did not remember the exact date when symp-
The patient was studied with cerebral magnetic reso-
toms began, but reported that they started approxi-
nance imaging (MRI) using paramagnetic contrast.
mately 4 or 5 years before our consultation.During those
Different pulse sequences were applied with a General
years she consulted lots of other physicians without
Electric Signa superconductive magnet of 1.5 Tesla
satisfactory results.She experienced between six and
equipment.Axial, coronal and saggital images were
seven episodes a day.The temporal pattern was about
made in T1 y T2.Paramagnetic contrast was also given
three or four times per week; of course this pattern was
to the patient. She was examined using F.L.A.I.R. effect,
related to exposition to pain triggers that she had
saggital T1 effect and Fast Spin ECO T2.We also
identi®ed.Each one consisted of an abrupt and intense
performed spectroscopic and perfusion studies.
peak of 30±45 s, followed by a painful burning feeling
The Fast Spin ECO T2 (Fig.1) study showed absence
that lasted for 35 min to 2 h.The after-attack burning
of demyelinating lesions in the axial as well as in
the coronal series.The region of the cerebellopontine
The neuralgic pain began in the medial canthus of
angle was free of expansive processes.We observed an
the right eye, involving later a triangular orbitofrontal
important change in a superior cerebellar artery root.
area and, with less intensity, the upper half of her
This vessel made contact with the right trigeminal nerve
right cheek.During the peak of the pain there was ocular
that appeared toned down (Figs 1, 2 and 3).
congestion, tearing, oedema (observed only in the eye-
lids) and ipsilateral palpebral ptosis.Crises were not
only spontaneous, but also were triggered by touching
the periorbital area, brushing her teeth, yawning, chew-
Under the effects of general anaesthesia with endo-
ing and washing her hair.In addition, exposure to strong
tracheal intubation and ECG, arterial pressure and
# Blackwell Science Ltd Cephalalgia, 2001, 21, 996±999
Figure 3 MRI axial T1WI: vascular structure (arrow) touching
Figure 1 In the FAST SPIN ECHO effect a vascular structure
the trigeminal nerve (with hyper-intense ¯ow signal in
can be observed, like empty signal (arrow), in close relationship
Figure 4 In this ®gure the trigeminal nerve can be seen
(full arrow) entering into the pons.At this level it is being
fenestrated by a branch (small empty arrow) of the superior
cerebellar artery (big empty arrow).
the cerebellum.Once the Dandy's petrous vein wasfound, it was coagulated and cut, which allowed us to
Figure 2 MRI Coronal plain: appreciable vascular structure
(arrow) in contact with the right trigeminal nerve.
identify the ®fth cranial nerve in a vertical position,between the tentorium and the petrous bone, penetratingits border towards Gasser's ganglion.
gasometry monitoring, on left lateral decubitus (park
Focusing on an area rather proximate to the entry zone
bench position), a right suboccipital retro-mastoid cran-
of this cranial nerve into the pons (Fig.4, fenesmacro)
iectomy was performed.The duramatter was opened
we noticed that a superior cerebellar artery branch
in a semicircular shape following the latero-sigmoid
penetrated into the trigeminal nerve and fenestrated it.
sinus limits, exposing the superior and later faces of
This artery branch was dissected and separated from the
# Blackwell Science Ltd Cephalalgia, 2001, 21, 996±999
reported in the literature.This syndrome has some
similarities with cluster headache (17) and ®rst-division
trigeminal neuralgia.A great many medical treatments
(18) with uncertain results are proposed in order to
diminish the intensity or the duration of the symptoms.
By means of the neuroimaging techniques we have
employed, an important change in a superior cerebellar
artery root was oberved.This vessel contacted with the
right trigeminal nerve.Because of the lack of bene®ts
brought by the large number of medical treatments tried
with this patient, we proposed a surgical treatment with
the `Jannetta technique' (microvascular decompression),
which is frequently used to treat trigeminal neuralgia.
The purpose of this technique is to separate an artery
branch, or more rarely a vein, in close relationship with
Figure 5 In this photo, the fenestrating artery branch (small
the entry zone of the ®fth cranial nerve into the pons.
empty arrow) is disjoining from the superior cerebellar artery
In the case we report (Figs 1, 2 and 3) we found
(big empty arrow) perpendicularly.It has just been separated
from the fenestration of the trigeminal nerve (full arrow).
a vascular compression of the trigeminal nerve in the
neuroradiological images, similar to that found in the
essential neuralgias successfully treated with this proce-
dure.This should be, according to our knowledge, the
third case in the literature of a SUNCT syndrome treated
with surgical procedures.The ®rst (20) was treated with
a similar technique and the other (21) with a per-
cutaneous compression of the Gasser's ganglion.The
present case stands as a new option in the therapeutic
management of SUNCT syndrome.This case, success-
fully treated with a surgical procedure, should encour-
age neurologists to require neuroradiological studies
with the purpose of evidencing a neurovascular com-
pression.Consequently, when medical treatment is not
successful, this surgery, performed by professionals with
proven experience in this ®eld, becomes a possible
choice with minimal morbidity or mortality.
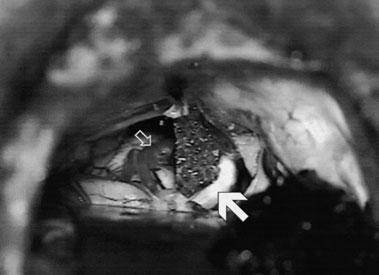
Figure 6 Final position: a foam rubber sponge is placed
between the fenestrating vessel (empty arrow) and the nerve
(full arrow), precluding the direct contact of both structures.
nerve, retracting it from the nerve fenestration (Fig.5,
1 Sjaastad O, Saunte C, Salvesen R et al.Shortlasting, unilateral
sin fenesmicro).A foam rubber sponge was placed
neuralgiform headache attacks with conjunctival injection,
between both structures (Fig.6, esponga 3).The dura-
tearing, sweating, and rhinorrhea.Cephalalgia 1989; 9:147±56.
matter and the other plains were closed in accordance
2 Sjaastad O, Zhao J-M, Kruszewski P, Stovner L-J.Shortlasting,
unilateral, neuralgiform headache attacks with conjunctivalinjection, tearing, etc.(SUNCT): III.Another Norwegian case.
The patient stayed in the intensive care unit for
12 h, and then spent 2 days in the general care room.
3 Kruszewski P, Fasano ML, Brubakk AO, Shen JM, Sand T,
She left hospital on the third day with total pain relief.
Sjaastad O.Shortlasting, unilateral, neuralgiform headache
The patient has remained asymptomatic and there was
attacks with conjunctival injection, tearing, and subclinical
no recurrence up to now, 17 months after the surgery.
forehead sweating (`Sunct' syndrome).II.Changes in heartrate and arterial blood pressure during pain paroxysms. Headache 1991; 31:399±405.
4 Pareja JA, Sjaastad O.SUNCT syndrome in the female.
5 Sjaastad O, Kruszewski P.Trigeminal neuralgia and SUNCT
Ottar Sjaastad decribed the ®rst case of SUNCT syn-
syndrome: similarities and differences in the clinical pictures.
drome in 1978 (1).Since then, many cases have been
An overview.Funct Neurol 1992; 7:103±7.
# Blackwell Science Ltd Cephalalgia, 2001, 21, 996±999
6 Bouhassira D, Attal N, Esteve M, Chauvin M.SUNCT
syndrome.A case of transformation from trigeminal
headache attacks with conjunctival injection and tearing
neuralgia? Cephalalgia 1994; 14:168±70.
(SUNCT syndrome): V.Orbital phlebography.Cephalalgia
7 Kruszewski P, Zhao JM, Shen JM, Sjaastad O.SUNCT
syndrome: forehead sweating pattern.Cephalalgia 1993;
15 Sjaastad O, Kruszewski P, Fostad K, Elsis T, Qvigstad G.
SUNCT syndrome.VII.Ocular and related variables.
8 Becser N, Berky M.SUNCT syndrome: a Hungarian case.
16 Zhao JM, Sjaastad O.SUNCT syndrome.VIII.Pupillary
9 Pareja JA, Pareja J, Palomo T, Caballero V, Pamo M.SUNCT
reaction and corneal sensitivity.Funct Neurol 1993; 8:409±14.
syndrome: repetitive and overlapping attacks.Headache
17 Headache Classi®cation Committee of the International
Headache Society.Classi®cation and diagnostic criteria for
10 Bussone G, Leone M, Dalla Volta G, Strada L, Gasparotti R,
headache disorders cranial neuralgias and facial pain.
Di Monda V.Short-lasting unilateral neuralgiform headache
Cephalalgia 1988; 8 (Suppl.7):1±96.
attacks with tearing and conjunctival injection: the ®rst
18 Pareja JA, Kruszewski P, Sjaastad O.SUNCT syndrome:
`symptomatic' case? Cephalalgia 1991; 11:123±7.
trials of drugs and anesthetic blockades.Headache 1995;
11 Morales F, Mostacero E, Marta J, Sanchez S.Vascular
malformation of the cerebellopontine angle associated
19 Raimondi E, Gardella LA.SUNCT syndrome.Two cases in
with `SUNCT' syndrome.Cephalalgia 1994; 14:301±2.
Argentina.Headache 1998; 38:369±71.
12 Hannerz J, Greitz D, Hansson P, Ericson K.SUNCT may be
20 Lenaerts M, Diederich N, Phuce K.A patient with SUNCT
another manifestation of orbital venous vasculitis.Headache
cured by the Jannetta procedure.Poster presentations, Session
IV, 460, 8th Congress of the IHS.Cephalalgia 1997; 17.
13 Wober C, Wober-Bingol C, Wessley P.Das SUNCT syndrom.
21 Morales-AsõÂn F, Espada F, LoÂpez-Obarrio LA, Navas I,
Fallbericht und Literaturubersicht.Fortschr Neuro Psychiatr
Escalza I, InÄõÂguez C.A SUNCT case with response to
surgical treatment.Cephalalgia 2000; 20:67±8.
# Blackwell Science Ltd Cephalalgia, 2001, 21, 996±999

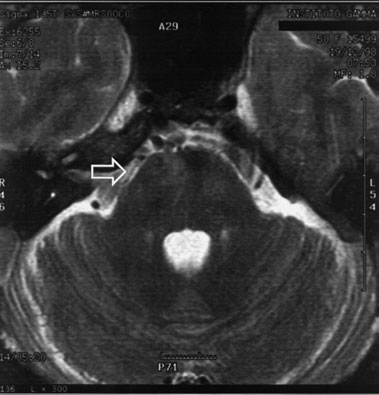

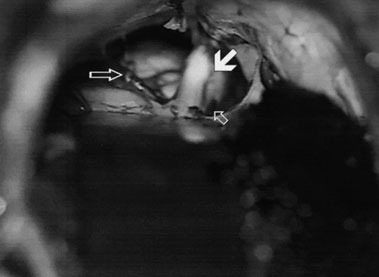 Figure 3 MRI axial T1WI: vascular structure (arrow) touching
Figure 1 In the FAST SPIN ECHO effect a vascular structure
the trigeminal nerve (with hyper-intense ¯ow signal in
can be observed, like empty signal (arrow), in close relationship
Figure 4 In this ®gure the trigeminal nerve can be seen
(full arrow) entering into the pons.At this level it is being
fenestrated by a branch (small empty arrow) of the superior
cerebellar artery (big empty arrow).
Figure 3 MRI axial T1WI: vascular structure (arrow) touching
Figure 1 In the FAST SPIN ECHO effect a vascular structure
the trigeminal nerve (with hyper-intense ¯ow signal in
can be observed, like empty signal (arrow), in close relationship
Figure 4 In this ®gure the trigeminal nerve can be seen
(full arrow) entering into the pons.At this level it is being
fenestrated by a branch (small empty arrow) of the superior
cerebellar artery (big empty arrow).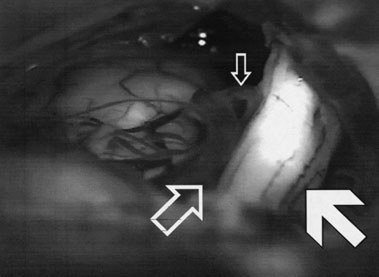
 reported in the literature.This syndrome has some
similarities with cluster headache (17) and ®rst-division
trigeminal neuralgia.A great many medical treatments
(18) with uncertain results are proposed in order to
diminish the intensity or the duration of the symptoms.
reported in the literature.This syndrome has some
similarities with cluster headache (17) and ®rst-division
trigeminal neuralgia.A great many medical treatments
(18) with uncertain results are proposed in order to
diminish the intensity or the duration of the symptoms.