Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Gicasym.org
Role of NSAIDs in the Adjuvant Therapy of Colon Cancer Charles S. Fuchs, MD, MPH Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA
Experimental, epidemiologic, and clinical data provide rectal cancer, regular aspirin or selective COX-2 inhibitor
strong evidence for a causative link between chronic
use conferred a signifıcant improvement in survival, and this
inflammation and colorectal cancer (CRC) risk, including
benefıt was greatest in patients whose tumors overexpressed
the well-described association between inflammatory bowel
COX-2. In the fırst study, we prospectively assessed aspirin
disease and colonic dysplasia. Inflammation predisposes to
use in 1,279 men and women diagnosed with stage I, II, or III
cancer through enhanced cellular proliferation and mu-
colorectal cancer, with a median follow-up of 11.8 years.6
tagenesis, inability to adapt to oxidative stresses, promotion
Compared with nonusers, participants who regularly used
of angiogenesis, inhibition of apoptosis, and secretion of
aspirin after the diagnosis of colorectal cancer experienced a
mediators that may promote tumorigenesis.1 One specifıc
multivariate HR for colorectal cancer–specifıc mortality of
mechanism through which inflammation leads to both
0.71 (95% CI, 0.53-0.95) and for overall mortality of 0.79
colitis-associated and sporadic carcinogenesis is the pro-
(95% CI, 0.65-0.97). Of note, the effect of aspirin differed
inflammatory cyclooxygenase (COX) pathway.
signifıcantly according to COX-2 expression (p value for in-
Observational studies and randomized clinical trials
teraction ϭ 0.04). Regular aspirin use after diagnosis was as-
(RCTs) fınd that aspirin, nonsteroidal anti-inflammatory
sociated with a lower risk of colorectal cancer–specifıc
drugs, and selective COX-2 inhibitors reduce CRC and ad-
mortality among participants in whom primary tumors
enoma risk. In four randomized, placebo-controlled trials of
overexpressed COX-2 (multivariate HR, 0.39; 95% CI, 0.20-
patients who had undergone a colonoscopic resection of an
0.76), whereas aspirin use was not associated with lower risk
adenomatous polyp, daily aspirin conferred a signifıcant re-
among those with primary tumors with weak or absent ex-
duction in the risk of recurrent adenomas at 3 years (relative
pression (multivariate HR, 1.22; 95% CI, 0.36-4.18).
risks [RRs] 0.61-0.83).2 In the British Doctors Aspirin Trial
In an independent study of patients with stage III colon
(7,588 participants followed for more than 20 years), sub-
cancer enrolled in a National Cancer Institute (NCI)-
jects randomly assigned to aspirin experienced a 26% reduc-
sponsored cooperative trial of adjuvant chemotherapy
tion in the risk of developing colorectal cancer compared
(CALGB 89803), we prospectively assessed the influence of
with those receiving placebo (hazard ratio [HR] ϭ 0.74; 95%
aspirin and selective COX-2 inhibitor use on patient out-
come.7 Patients with stage III colorectal cancer reporting
To defıne potential mechanisms by which aspirin affects
consistent aspirin use experienced an adjusted HR of 0.46
colon carcinogenesis, we estimated COX-2 expression by
(95% CI, 0.23-0.95) for disease-free survival (DFS) and 0.49
immunohistochemistry in CRC specimens from two large
(95% CI, 0.19-1.30) for overall survival. Moreover, users of
prospective cohorts of healthy participants who provided
either celecoxib or rofecoxib (5% of the cohort) experienced
data on aspirin use from a questionnaire every 2 years.4 Of
an HR for DFS of 0.47 (95% CI, 0.17-1.28) when compared
the 636 incident colorectal cancers, 423 (67%) had COX-2
to nonusers. These observational studies suggest that,
overexpression. The effect of aspirin use differed signifı-
among patients with stage I to III colorectal cancer, regular
cantly in relation to COX-2 expression (p value for hetero-
aspirin or selective COX-2 inhibitor use may substantially
geneity ϭ 0.02). Regular aspirin use conferred a signifıcant
improve both cancer-specifıc and overall survival.
reduction in the risk of colorectal cancers that overexpressed
Based on results from those studies, NCI-sponsored coop-
COX-2 (multivariate relative risk, 0.64; 95% CI, 0.52-0.78),
erative group investigators initiated a placebo-controlled
whereas regular aspirin use had no influence on tumors with
RCT assessing the influence of celecoxib on survival in 2,500
weak or absent expression of COX-2 (multivariate relative
patients with stage III colon cancer concurrently receiving
risk, 0.96; 95% CI, 0.73-1.26). These fındings strongly sup-
standard adjuvant therapy (CALGB/SWOG 80702; Fig. 1).
port the primacy of inhibition of COX-2–mediated synthe-
Four to eight weeks following a curative surgical resection of
sis of prostaglandins in the prevention of colon cancer.5
stage III colon cancer, patients are being randomized in a 2 x
Consistent with the apparent role of COX-2 in colorectal
2 design to (a) 5-fluorouracil, leucovorin, and oxaliplatin
carcinogenesis, three placebo-controlled RCTs demon-
(FOLFOX) for 3 months versus FOLFOX for 6 months and
strated that celecoxib or rofecoxib signifıcantly reduced ad-
(b) celecoxib (400 mg per day for 3 years) versus placebo
enoma risk in patients with prior polyps (RRs 0.55-0.76; all
once per day for 3 years. Celecoxib or placebo is initiated on
the fırst day of chemotherapy. The primary objective of the
Beyond cancer prevention, animal models of established
trial is to compare DFS for celecoxib versus placebo, and
colorectal cancers demonstrate that COX-2 inhibitors can
with 2,500 subjects enrolled and 775 events expected at anal-
reverse tumor growth. In two studies of patients with colo-
ysis, there is 91% power (two-sided ␣ ϭ 0.05) to detect an
Fig. 1. CALGB 80702 trial design.
HR of 0.79 in favor of celecoxib. A secondary endpoint is to
(3) categorizing tumors based on molecular subtypes (e.g.,
compare DFS for 3 months versus 6 months of chemother-
COX-2, NF-, -catenin expression) and examining cele-
apy. Overall survival and treatment-related toxicity are also
coxib in relation to these phenotypes, based on hypothesized
relations. Such analyses provide further evidence for causal-
CALGB/SWOG 80702 will provide invaluable insight into
ity, offer critical mechanistic insight, and, most importantly,
the influence of inflammation and interventions that target
defıne populations most likely to benefıt from interventions
inflammation on patient outcome in stage III colon cancer,
targeting these pathways. Thus, the results of this trial may
including the following: (1) utilizing the largest RCT, where
improve our understanding of CRC biology, identify new
patient, disease, and treatment characteristics are well con-
means to improve patient survival, and, with the extensive
trolled and disease follow-up is uniformly conducted, to
clinical, pathologic, genomic, and biomarker data available
evaluate the effect of COX-2 inhibition and inflammation on
for analysis, inform clinicians how to maximally utilize
patient survival; (2) leveraging the resources of this RCT and
inflammatory-targeted interventions to improve clinical
incorporating prospective collection of lifestyle habits, base-
line germ-line DNA, plasma, and tumor specimens; and
DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Relationships are considered self-held and compensated unless otherwise noted. Relationships marked “L” indicate leadership positions. Relationships marked “I” are those held by an immediatefamily member; those marked “B” are held by the author and an immediate family member. Relationships marked “U” are uncompensated. Employment or Leadership Position: None. Consultant or Advisory Role: Charles S. Fuchs, Amgen; AstraZeneca; Genentech; Genomic Health; ImClone Systems; Merck; Metamark Genetics; Pfizer; Roche; Sanofi. Stock Ownership: None. Honoraria: None. Research Funding: None. Expert Testimony: None. Other Remuneration: None. REFERENCES
1. Schottenfeld D, Beebe-Dimmer J. Chronic inflammation: a common and im-
5. Markowitz SD. Aspirin and colon cancer—targeting prevention? N Engl J Med.
portant factor in the pathogenesis of neoplasia. CA Cancer J Clin. 2006;56:
6. Chan AT, Ogino S, Fuchs CS. Aspirin use and survival after diagnosis of
2. Chan AT, Giovannucci EL. Primary prevention of colorectal cancer. Gastroen-
colorectal cancer. JAMA. 2009;302:649-658.
7. Fuchs C, Meyerhardt JA, Heseltine DL, et al. Influence of regular aspirin use
3. Flossmann E, Rothwell PM. Effect of aspirin on long-term risk of colorectal
on survival for patients with stage III colon cancer: Findings from intergroup
cancer: consistent evidence from randomised and observational studies.
trial CALGB 89803. J Clin Oncol. 2005;23 (suppl; abstract 3530).
4. Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in
relation to the expression of COX-2. N Engl J Med. 2007;356:2131-2142.
2013 GASTROINTESTINAL CANCERS SYMPOSIUM PROCEEDINGS
One month into 2008 … have room for one more resolution? How about: "Avoid litigationthis year"? Here is a brief update of some recent developments in the areas of intellectualproperty, commercial and employment lawand some practical advice as to what youcan do now to avoid litigation in the future. Ifyou are already facing litigation, these tipsmay benefit your litigation strategy or h
Gebrauchsinformation Liebe Patientin, lieber Patient! Bitte lesen Sie diese Gebrauchsinformation aufmerksam, weil sie wichtige Informationen darüber enthält, was Sie bei der Anwendung dieses Arzneimittels beachten sollen. Wenden Sie sich bei Fragen bitte an Ihren Arzt oder Apotheker. Ginseng G 500 mg Ginsengwurzel-Pulver, 100 mg natives Weizenkeimöl, 400 mg Färberdistelöl. Sojal
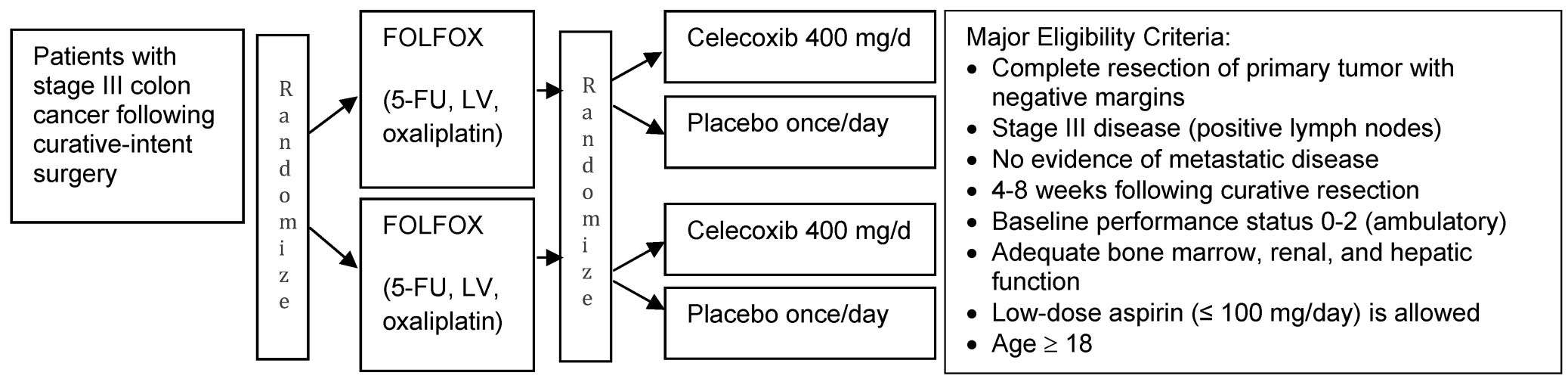 Fig. 1. CALGB 80702 trial design.
Fig. 1. CALGB 80702 trial design.