Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Update: clinically significant cytochrome p-450 drug interactions
Update: Clinically Significant Cytochrome P-450 Drug Interactions
Elizabeth Landrum Michalets, Pharm.D.
Recent technologies have resulted in an explosion of information concerning the cytochrome P-450 isoenzymes and increased awareness of life-threatening interactions with such commonly prescribed drugs as cisapride and some antihistamines. Knowledge of the substrates, inhibitors, and inducers of these enzymes assists in predicting clinically significant drug interactions. In addition to inhibition and induction, microsomal drug metabolism is affected by genetic polymorphisms, age, nutrition, hepatic disease, and endogenous chemicals. Of the more than 30 human isoenzymes identified to date, the major ones responsible for drug metabolism include CYP3A4, CYP2D6, CYP1A2, and the CYP2C subfamily. (Pharmacotherapy 1998;18(1):84–112)
Significant Inhibitory Interactions: Protease
Significant Induction Interactions: Protease
Significant Induction Interactions: Estrogens and
Significant Inhibitory Interactions: Antihistamines
Significant Inhibitory Interactions: Cisapride
Significant Inhibitory Interactions: Corticosteroids
Significant Inhibitory Interactions: R-Warfarin
Significant Inhibitory Interactions: Antidepressants
Significant Induction Interactions: Benzodiazepines
Significant Induction Interactions: Narcotic
Significant Inhibitory Interactions: Cardiovascular
Significant Inhibitory Interactions: Narcotic
Significant Induction Interactions: Calcium Channel
Significant Inhibitory Interactions: Theophylline
Significant Induction Interactions: Theophylline
Significant Inhibitory and Induction Reactions:
Significant Inhibitory Interactions: R-Warfarin
Significant Inhibitory Interactions: Antidepressants,
Significant Induction Interactions: Benzodiazepines
From the Department of Pharmacy, Mission–St. Joseph’s
Health System, and the University of North Carolina School
Significant Inhibitory Interactions: Phenytoin
of Pharmacy Community-Based Practice, Asheville, North
Significant Induction Interactions: Phenytoin
Significant Inhibitory Interactions: S-Warfarin
Address reprint requests to Elizabeth Landrum Michalets,
Significant Induction Interactions: S-Warfarin
Pharm.D., Department of Pharmacy, Mission–St. Joseph’sHealth System, 509 Biltmore Avenue, Asheville, NC 28801.
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsNomenclature
one isoenzyme. For example, the pharmacologicallyactive enantiomer S-warfarin is metabolized by
The cytochrome P (CYP)-450 isoenzymes are a
group of heme-containing enzymes embedded
primarily in the lipid bilayer of the endoplasmic
systems.7, 8 Therefore, when one enzyme system
reticulum of hepatocytes (Figure 1).1 Thesemetabolic enzymes are also present in high
is inhibited or induced by an interacting drug, a
concentrations in enterocytes of the small
clinically significant interaction may or may not
intestine, with smaller quantities in extrahepatic
occur. Another example is tricyclic antidepressants,
tissues (kidneys, lungs, brain). They are
which are metabolized by CYP2D6, CYP1A2, and
involved in oxidative metabolism (phase I) of a
CYP3A4. Inhibition or genetic absence of one
number of different drug classes as well as endo-
isoenzyme can lead to compensation through the
genous substances such as steroid hormones,
secondary isoenzyme pathway. Similar to warfarin,
fatty acids, and prostaglandins.2–4 The nomenclature
oxidative metabolism can be preserved, and a
first suggested by Nebert et al in 1987 and widely
clinically significant interaction may or may not
used today employs a three-tier classification
consisting of the family (> 36% homology in
In addition, a drug may inhibit or induce the
amino acid sequence), subfamily (77% homology),
activity of a specific isoenzyme even though it is
not a substrate at that particular site. For example,
Knowledge of the substrates, inhibitors, and
quinidine is metabolized by the CYP3A4 enzyme,
inducers of CYP-450 isoenzymes assists in
but it is a potent inhibitor of CYP2D6.2, 10
predicting clinically significant drug interactions. It is also important to recognize that genetic
polymorphism in the functional expression of
Inhibition most often occurs as a result of
competitive binding at the enzyme’s binding site.
contributes to marked interpatient variability in
Competitive inhibition depends on the affinity of
drug metabolism, leading to poor metabolizers
the substrate for the enzyme being inhibited, the
(PMs) and extensive metabolizers (EMs).2, 3, 6 In
addition to genetic influences, microsomal drug
inhibition, and the half-life of the inhibitor drug.
metabolism is affected by age, nutrition, stress,
The onset and offset of enzyme inhibition are
dependent on the half-life and time to steady
endogenous chemicals.1 Although more than 30
state of the inhibitor drug. For example,
human CYP-450 isoenzymes have been identified
to date, the major ones responsible for drug
ingestion, and cimetidine (CYP1A2) inhibit drug
metabolism are CYP3A4, CYP2D6, CYP1A2, and
metabolism within 24 hours of a single dose, but
amiodarone (CYP2C9) inhibitory interactionsmay not surface for months because of its long
Substrates, Inhibition, and Induction
Some drugs may be metabolized by more than
The time to maximum drug interaction (onset
Figure 1. Cytochrome P-450 enzyme system. Reprinted by permission from Applied Pharmacokinetics: Principles of Therapeutic Drug Monitoring, third edition, edited by WE Evans, JJ Schentag, and WJ Jusko, published by Applied Therapeutics, Inc., Vancouver, WA, 1992.
PHARMACOTHERAPY Volume 18, Number 1, 1998
and termination) is also dependent on the time
Both of these agents interact with warfarin
required for the inhibited drug to reach a new
metabolism. Whereas rifampin’s effects occur
steady state.6, 12 For example, with the cimetidine-
within 4 days, phenobarbital’s effects take 14–22
theophylline interaction, maximum increases in
theophylline concentrations are not seen for
A complicating factor is that the time course of
approximately 2 days, since this time is required
induction is also dependent on the time required
for theophylline to reach a new steady state.13
production. In other words, the rate-limiting
concentration-dependent half-life, steady-state
factor may be the half-life of CYP450 enzyme
changes in phenytoin serum concentration can
turnover, which ranges from 1–6 days.17 Since
take days to occur. Of interest, if the half-life of
rifampin is eliminated more rapidly than the
the inhibitor drug is shorter than that of the
excess cytochrome enzymes, the rate-limiting
inhibited drug, less time is required to revert to a
factor in the duration of the interaction would be
lower steady-state concentration after the
enzyme turnover. With phenobarbital, accumu-
inhibitor is stopped than is required to increase
lation and elimination would be the rate-limiting
to a new steady-state concentration when the
factor in the onset and offset of induction.17
inhibitor is started. This is because the half-life
Enzyme induction is also influenced by age
of the affected drug is shorter after discontinuation
and liver disease. The ability to induce drug
metabolism may decrease with age, as evidenced
by reports that drug metabolism in elderly subjects
inhibition is noncompetitive, which can occur as
(> 60 yrs) is not influenced by polycyclic aromatic
a result of inhibitor inactivation of the enzyme
hydrocarbons (PAH) in cigarette smoke, as it is in
with normal substrate binding. The duration of
younger subjects.1, 18 Also, patients with cirrhosis
this type of inhibition may be longer if new
or hepatitis may be less susceptible to enzyme
enzymes are synthesized after the inhibitor drug
Another contributing factor to the significance
CYP3A4 Isoenzyme
of enzyme inhibition is the hepatic extraction
The CYP3A4 isoenzyme is responsible for the
ratio of the affected drug. In general, systemic
metabolism of the widest range of drugs and
clearance of low-extraction-ratio drugs is
endogenous compounds in humans. It accounts
expected to be affected to a greater extent than
for 60% of cytochrome enzymes in the liver and
that of high-extraction-ratio drugs. However,
70% of those in enterocytes found in the gut wall
with high-extraction-ratio drugs with significant
responsible for first-pass metabolism.2, 3, 17 No
first pass metabolism, it is well known that
evidence to date suggests the 3A4 isoenzyme
significant changes in oral absorption can occur
substrates, inhibitors, and inducers of CYP3A4are listed in Table 1.2, 3, 9, 10, 16, 17, 19–117
In recent years there has been an explosion of
Enzyme induction, first recognized in the
discussion about the 3A4 system because of life-
threatening arrhythmic side effects that can occur
increased or the synthesis of more CYP-450
as a result of enzyme inhibition and accumulationof the nonsedating antihistamines terfenadine
and astemizole20–25 and cisapride.26–30
phenobarbital increases liver weight in a dose-dependent manner. In humans, liver biopsies inpatients taking anticonvulsants resulted in up to
Significant Inhibitory Interactions: Antihistamines
52% larger absolute liver size.14 Like inhibitors,
Terfenadine has been removed from the market
inducers tend to be lipophilic, and the time
because of its serious cardiovascular drug
course of the interaction is dependent on the
interactions. Its active carboxy metabolite,
half-life of the inducer. For example, rifampin’s
fexofenadine, is available and devoid of the fatal
short half-life results in enzyme induction
drug interactions.31 Astemizole undergoes
(CYP3A4, CYP2C) apparent within 24 hours,
extensive first-pass metabolism to active
whereas phenobarbital’s longer half-life of 3–5
metabolites, and, like terfenadine, the parent
days requires approximately 1 week for induction
compound is the cardiotoxic entity.32 In many
(CYP3A4, CYP1A2, CYP2C) to become apparent.
cases, drug interactions with terfenadine have
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsTable 1. Cytochrome 3A4 Isoenzyme: Substrates, Inducers, and Inhibitors2, 3, 9, 10, 16, 17, 19–117 Substrates
been extrapolated to astemizole.31 Terfenadine,
serious nature of potential drug interactions,
available since 1985, was first reported in 1990 to
cause QT prolongation and torsades de pointes
candidiasis are not likely to present a problem.
when given together with ketoconazole.23 A
The new antifungal terbinafine does not appear
prospective study of six healthy volunteers given
to inhibit the 3A4 system and is an alternative for
the combination noted increased parent terfenadine
concentrations and QT prolongation (mean 82-
Erythromycin alone can cause QT prolongation,119
and when combined with terfenadine does so as
In vitro, the ability of itraconazole, an anti-
well (mean 10-msec increase) but to a lesser degree
fungal similar to ketoconazole, to inhibit the 3A4
than when given with antifungal agents.20 This
system is 10 times less potent than that of
effect was also reported with clarithromycin31 but
ketoconazole, but inhibitory differences in vivo
not with azithromycin or dirithromycin, which
are less impressive.33 Fluconazole also inhibits
may be alternatives for patients receiving
3A4 in vitro, but did not increase parent
terfenadine concentrations or cause arrhythmias
In vitro evidence exists for inhibition of the
at dosages of 200 mg/day.32 However, dosages
3A4 isoenzyme by the antidepressant drugs
above 200 mg/day caused QT prolongation in
sertraline. In addition, plasma concentrations of
The antifungal agents itraconazole, ketoconazole,
drugs metabolized by 3A4 such as carbamazepine
fluconazole, and intravenous miconazole should
and some benzodiazepines increased when given
not be coadministered with astemizole due to the
concomitantly with these four agents.9, 19, 39, 40 To
PHARMACOTHERAPY Volume 18, Number 1, 1998
date, there are no in vitro data or case reports
contraindicated with astemizole since the
involving paroxetine in the inhibition of 3A4.19
combination may result in QT prolongation.58 It
Data on significant drug interactions with these
is prudent to limit the use of quinine and tonic
antidepressants and antihistamines is less clear
water in patients receiving astemizole.
than with antifungals and macrolides. Fluoxetine
In vitro, the protease inhibitors saquinavir,
caused arrhythmias in patients concomitantly
ritonavir, indinavir, and nelfinavir inhibit cyto-
receiving terfenadine.41, 42 Another concern with
chrome 3A4.59 To date, neither pharmacokinetic
fluoxetine is the long half-life of the parent
studies nor in vivo drug-drug interaction studies
compound (4–6 days) and its active metabolite
have been conducted for these agents with
norfluoxetine (4–16 days). The consequences of
antihistamines. Prescribing information for
an interaction may be minimized by delaying
ritonavir60 lists concomitant administration with
administration of astemizole for 2–4 weeks after
astemizole as a contraindication, and prescribing
discontinuing fluoxetine.43 Prescribing infor-
information for saquinavir,61 indinavir,62 and
mation for both fluvoxamine and nefazodone
lists concomitant administration with astemizole
concomitant astemizole administration because
as a contraindication,44–46 and sertraline information
of the potential for life-threatening cardiotoxic
warns against concomitant administration with
astemizole.47 Thus, fluoxetine, fluvoxamine,
Other recommendations to minimize the risk
nefazodone, and sertraline should be administered
of cardiotoxic drug interactions include avoiding
cautiously, if at all, to patients taking astemizole
astemizole dosages greater than 10 mg/day,
(Table 2).2, 3, 7–11, 14–118 In patients receiving
prescribing alternative agents (Table 2),
astemizole, alternatives for the treatment of
prescribing astemizole cautiously in patients with
depression are paroxetine19 and venlafaxine.48 The
cardiac conditions that predispose them to QT
tricyclic antidepressants should also be prescribed
prolongation, administering the drug cautiously in
cautiously since they can cause arrhythmias.9
patients taking other agents that can prolong the
Fresh or frozen grapefruit juice inhibits
QT interval (e.g., type Ia or III antiarrhythmics;
inhibitory substance was once thought to be
droperidol, tricyclic antidepressants), and
naringenin, a human metabolite of nargingin.49–51
administering astemizole cautiously in patients
However, the primary substance responsible for
inhibition was identified in vitro to be a furano-coumarin compound widely found in nature, 6,7-
Significant Inhibitory Interactions: Cisapride
dihydroxybergamottin. This inhibitory substanceis less potent than ketoconazole but considerably
The fact that cisapride can cause tachycardia,
more active than cimetidine. Lack of 6,7-
palpitations, and extrasystoles was first observed
dihydroxybergamottin in orange juice probably
in a review of records of over 13,000 patients
receiving the agent.28 Postulations about the
inhibitory effects.52–54 Inhibition of terfenadine
cause of tachycardia include activation of
metabolism with quantifiable levels of the
serotonin-4 receptors on the myocardium63 and
terfenadine parent compound, an increase in area
prolonged atrioventricular conduction due to its
under the curve (AUC) of 55%, and a mean QT
structural similarity to procainamide.30 The first
report of an arrhythmic drug interaction with
patients ingesting grapefruit juice 240 ml
cisapride was with erythromycin (for 2 days
only) with dosages of cisapride that were rapidly
twice/day.55, 56 Other studies reported similar
escalated to 40 mg every 6 hours. The patient
pharmacokinetic changes but associated with no
developed a QT interval of 550 msec from a
normal baseline with progression to polymorphic
Recently the calcium channel blocker, mibefradil,
nonsustained ventricular tachycardia. The QT
has been shown to inhibit both CYP3A4 and
interval returned to normal after the cisapride
CYP2D6 and cause syncope in some patients taking
dosage was decreased to 5 mg every 6 hours.29
-blockers. Because mibefradil could theoretically
Janssen Pharmaceutica continues to receive
increase plasma concentrations of astemizole, its
numerous reports of torsades de pointes, prolonged
QT intervals, and deaths.27 Over 50% of these
Another cytochrome 3A4 inhibitor is quinine.
patients were concomitantly receiving ketoconazole,
At dosages greater than 430 mg/day, quinine is
itraconazole, or fluconazole, and erythromycin,
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsTable 2. 3A4 Clinically Significant Drug Interactions2–3, 7–11, 14–118
on starting or stopping; may alsobe 1A2 mediated.
dose related; monitor INR morecarefully.
tremor in some patients;monitor SC&E.
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 2. 3A4 Clinically Significant Drug Interactions2, 3, 7–11, 14–118 (continued)
clinical response reported;fluconazole less affected.
LoratadineaMetoclopramideaAzithromycinDirithromycin
Ketoconazole (inh)Miconazole i.v. (inh)Fluoxetine (inh)
Nefazodone (inh)Sertraline (inh)Grapefruit juice (inh)
Nelfinavir (inh)Ritonavir (inh)Saquinavir (inh)Mibefradil (inh)
35% increase in terfenadineconc reported with zileuton.
monitoring; no cardiac sideeffects reported.
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsTable 2. 3A4 Clinically Significant Drug Interactions2, 3, 7–11, 14–118 (continued)
higher initial dosages ofbenzodiazepine.
Nelfinavir (inh)Ritonavir (inh)Saquinavir (inh)Rifampin (ind)
increase; monitor clinicaleffects; best documentedwith diltiazem, verapamil,nifedipine.
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 2. 3A4 Clinically Significant Drug Interactions2, 3, 7–11, 14–118 (continued)
Erythromycin (inh)Cyclosporine (inh)Nifedipine (inh)Diltiazem (inh)
Doxorubicin (inh)Etoposide (inh)Ketoconazole (inh)Erythromycin (inh)
contraception for short courses;for long courses use higherdosages or medroxyprogesteroneacetate.
increase dosage to 50 µg estradiol.
Ritonavir (inh)Saquinavir (inh)Norfloxacin (inh)
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsTable 2. 3A4 Clinically Significant Drug Interactions2, 3, 7–11, 14–118 (continued)
azole; monitor trough concmore carefully.
need dosage decrease;monitor trough conc.
53% with indinavir; decrease clarithromycin
dosage by 50% for Clcr 30–60 ml/min and
with rifampin and 50% with rifabutin;clinical significance unknown.
of icterus and uveitis; monitor forocular SE.
of icterus and uveitis; monitor forocular SE.
Ritonavir (inh)Saquinavir (inh)Rifampin (ind)
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 2. 3A4 Clinically Significant Drug Interactions2–3, 7–11, 14–118 (continued)
ritonavir AUC 35%; may needdosage increase; see specificMMWR guidelines.
150%; with ketoconazole, decreaseinitial indinavir dosage to600 mg q8h; decreasesaquinavir dosage ifketoconazole dosage is> 200 mg/day.
SC&E = serum concentration and effects; INR = international normalized ratio; SE = side effects; CCB = calcium channel blockers; BP = bloodpressure; HR = heart rate; BMT = bone marrow transplantation; F = bioavailability; Clcr = creatinine clearance; MAC = Mycobacterium aviumintracellulare complex; AUC = area under the concentration-time curve. aAlternative antihistamines and prokinetic agents in all interactions listed.
clarithromycin, or metronidazole. Risk factors
at baseline to 440 msec, and he died from
for arrhythmia were identified as history of
ventricular fibrillation-cardiac arrest. The drug
coronary disease and arrhythmia, renal insuf-
interaction was postulated as a potential culprit.
ficiency, electrolyte imbalance, and long-term use
Similar to antihistamines, only in vitro data
about enzyme inhibition, and no actual patient-
prolonged QT intervals such amiodarone and
specific data, are the bases for contraindications
and warnings against concomitant cisapride with
Three reports in our institution in 1995–1996
other drugs such as fluvoxamine, mibefradil,
involved fluconazole or erythromycin interactions
nefazodone, sertraline, ritonavir, saquinavir, and
with cisapride. Two patients were receiving both
indinavir.38, 44–46, 60–62 It would also seem prudent
fluconazole 100 and 400 mg/day and cisapride 20
to avoid administering fluoxetine, quinine, and
mg every 6 hours, had no known cardiac disease,
grapefruit juice with cisapride because of the fatal
developed ventricular fibrillation, and had
consequences of potential interactions, and
resolution with no further arrhythmias after
because similar interactions were documented
cisapride was discontinued. One of these patients
with terfenadine. As is the case with astemizole,
initially had recurrence of sustained ventricular
steps to minimize the cisapride drug interactions
tachycardia after lidocaine was discontinued and
include avoiding cisapride dosages greater than
before cisapride was discontinued. The third
20 mg every 6 hours and exercising caution in
patient had a history of cardiac disease and was
patients with hepatic disease or other risk factors
receiving erythromycin 500 mg intravenously
every 6 hours plus oral cisapride 10 mg every 12
Hypoprothrombinemic effects of warfarin were
hours. His QT interval increased from 352 msec
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
cisapride. The patient’s international normalization
diazepam and alprazolam, but enhancement of
ratio (INR) at baseline was 2.2–2.5 and increased
to 10.7, first noted 3 weeks after the patient
Another antidepressant, nefazodone, increased
began cisapride 10 mg 4 times/day. Competitive
alprazolam plasma concentrations 2-fold and
potentiated alprazolam-induced psychomotor
postulated.69 The clinical significance of this
impairment and sedation.71–74 Nefazodone also
interaction remains to be established.
increased triazolam plasma concentrations andhalf-life by 1.7- and 3-fold, respectively.71–73
Significant Inhibitory Interactions: R-Warfarin
Initial dosage reductions of alprazolam by 50%and triazolam by 75% should be made when
Fluconazole, itraconazole, and ketoconazole
adding nefazodone to existing therapy with these
reportedly increase the anticoagulant effects ofwarfarin. Two-fold (fluconazole) and 3-fold
(ketoconazole) increases in prothrombin time
Grapefruit juice 200 ml increased peak plasma
concentrations of orally administered midazolam
by 56% and AUC by 52%. The clinical importance
implicated to reduce the clearance of both
Temazepam, although metabolized by the 3A4
Numerous reports describe enhancement of the
system, does not result in significant pharmaco-
hypoprothrombinemic effects of warfarin when
kinetic or pharmacodynamic interactions as
given in combination with erythromycin.
Prothrombin times increased up to 2-fold after 7
inhibitors such as erythromycin and itraconazole.76, 77
days of therapy, but there are few reports of
Lack of interaction potential with temazepam
bleeding complications. The clinical relevance of
this interaction probably depends on many
triazolam may be due to different metabolic
patient factors including age, rate of warfarin
pathways and lack of significant first-pass
clearance, concurrent drug therapy, and ability to
shunt to noninhibited pathways.33 The inter-
reduced clearance of triazolam by 52% and
action has not been observed with azithromycin,
decreased midazolam clearance enough to cause
but like erythromycin, caution is advised with
unconsciousness. If it is not possible to avoid
these combinations, the benzodiazepine dosage
should be decreased by 50% and the patient
similar to the imidazole ring of cimetidine and
monitored carefully for respiratory depression
has been studied for inhibitory drug interactions.
and other signs of toxicity.36 Inhibitors of 3A4
It inhibits the metabolism of R-warfarin, and this
should therefore be administered with caution to
interaction is likely to be 3A4 mediated. The
patients taking alprazolam or triazolam and to
effects appear after omeprazole has been taken
those undergoing surgical procedures requiring
for a few days, seem to be dose related, and do
midazolam as a component of anesthesia.
not abate immediately on discontinuing the drug.
For the opioids, the only well-documented
3A4-mediated interaction is with alfentanil and
patients receiving this combination. Lansoprazole
erythromycin.70, 79 Reports include prolonged
does not alter the clearance of warfarin and may
respiratory depression associated with alfentanil
in patients who were receiving erythromycinbefore surgery.70 Administration of cimetidine
with fentanyl doubles the latter’s elimination half-
life, thus potentially enhancing its pharmacologiceffects and duration of action.70
Alfentanil, alprazolam, midazolam, temazepam,
and triazolam are among the currently known
substrates of cytochrome 3A4.9, 19, 39, 40, 72 The
benzodiazepines have fairly well documentedinteractions. Pharmacokinetic studies with
Rifampin can significantly impair the efficacy
alprazolam showed increased serum concentrations
of some benzodiazepines. A 96% reduction in
and prolonged half-life when given with the
nonexistent hypnotic effects when administered
Fluoxetine increased plasma concentrations of
with rifampin to 10 healthy volunteers in a
PHARMACOTHERAPY Volume 18, Number 1, 1998
double-blind crossover study.78 Similar results
As mentioned, HMG-CoA reductase inhibitors
were reported with triazolam and rifampin, with
are metabolized by the 3A4 system and have
markedly reduced effects of triazolam based on
dose-related toxic effects on skeletal muscle that
may range from diffuse myalgia and myopathy to
Like benzodiazepines, it is well known that
rifampin increases the rate of metabolism of
reported most frequently with lovastatin but have
also been reported rarely with the other statins.87,
greatest when HMG-CoA reductase inhibitors are
combined with 3A4 inhibitor drugs or agents that
compete with 3A4 metabolism.89–94 This inter-action has been well described with cyclosporine,
and less often with gemfibrozil and niacin.89
dependent on the 3A4 isoenzyme system for
In a double-blind, crossover trial, itraconazole
metabolism. Other cardiovascular drugs metab-
increased lovastatin peak concentrations by 20-
olized by 3A4 are the hydroxymethylglutaryl-
fold in 12 healthy volunteers. Side effects were
not reported in any subjects except one who
Grapefruit juice 200–250 ml given before drug
experienced a 10-fold increase in creatine
administration increased the AUC of felodipine
kinase.90 Reports of severe rhabdomyolysis
by 185%, with an average increase of 240%.
occurring after the addition of itraconazole to
Similar results occurred with nifedipine, nimodipine,
lovastatin and niacin therapy underscore the
and verapamil but not with diltiazem.50, 55
potential harm of these interactions. Myopathy
Furthermore, this pharmacokinetic interaction
also occurred after itraconazole was added to
was clinically significant, with lower diastolic
cyclosporine and simvastatin therapy in a
blood pressure, higher heart rate, and more
frequent vasodilation-related side effects with
described the development of rhabdomyolysis
felodipine, nisoldipine (5-fold increase in AUC),
when lovastatin was combined with erythromycin.
and nifedipine.55, 80, 81 This information supports
Myopathy is quickly reversible when the statin is
cautioning patients about concomitant ingestion
of grapefruit juice and calcium antagonists.
Concomitant administration of ritonavir and
A patient taking oral felodipine 10 mg/day was
lovastatin increased the AUC of lovastatin by 3-
given oral erythromycin 250 mg twice/day and
fold. Little information is available about
developed flushing, ankle and leg edema, and
protease inhibitors, but careful dosing with
tachycardia. When erythromycin was discon-
statins is prudent.58, 60–62 Giving statins with 3A4
tinued, felodipine levels were reduced from 6 to
inhibitors should be avoided or dosages of statins
less than 2 nmol/L and symptoms resolved.82 On
reduced to avoid the potential for rhabdomyolysis.
average, it appears that erythromycin increases
Patients should be instructed to monitor for signs
felodipine concentrations by 3-fold.55 Other
of myopathy such as muscular pain, tenderness,
studies have demonstrated similar increases in
or weakness, and plasma creatine kinase should
felodipine concentrations when given with
erythromycin.83 Other reports documentedsubstantial peripheral edema and/or elevated
Significant Induction Interactions: Calcium
calcium antagonist serum concentrations during
concurrent administration of itraconazole withfelodipine, isradipine, or nifedipine.84–86 An 8-
In one study, enzyme induction with rifampin
fold increase in feldopine’s AUC was seen when
resulted in up to a 32-fold increase in verapamil
the agent was given with itraconazole 200
clearance and a 25-fold decrease in verapamil
mg/day, and was associated with statistically
bioavailability after oral administration.95 The
significant changes in systolic and diastolic blood
effect of oral verapamil on atrioventricular
conduction was nearly abolished with rifampin
If concurrent therapy of potent 3A4 inhibitors
administration, and the authors concluded that
with calcium antagonists is required, the patient
prehepatic metabolism of verapamil was induced
should be monitored for signs of toxicity and the
by rifampin. Rifampin is expected to have a
dosage of calcium channel blocker decreased, if
similar reaction with other calcium channel
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
rifampin, carbamazepine, phenobarbital, andphenytoin are postulated to enhance efficacy and
Quinidine is known to be a cytochrome 2D6
toxicity through 3A4 activation. In immuno-
inhibitor but is metabolized by the 3A4 system.
histochemical studies, some patients with
Cytochrome 3A4 interactions that are well
pulmonary carcinoma showed expression of the
documented include those with cimetidine,2, 13
3A4 enzyme, and studies are continuing to assess
phenytoin, phenobarbital,2, 120 and rifampin.2, 114
if this presence leads to local activation and a
Of interest, metronidazole is a 3A4 inhibitor due
to its interaction with cisapride,27 and a potential
In contrast, inhibitors and other substrates of
interaction of quinidine with either metronidazole
3A4, such as ketoconazole, itraconazole, diltiazem,
verapamil, and cyclosporine, could possibly
difference in quinidine trough concentrations
interfere with activation and efficacy of
was noted, but with no changes in the patient’s
ifosfamide The clinical significance of inhibition
QT interval.10 An interaction with metronidazole
seems more likely since it is a known 3A4
In vitro, vinblastine metabolism is inhibited by
inhibitor. Quinidine concentrations should be
other anticancer drugs, including doxorubicin
monitored and patients assessed for signs of
and etoposide, together with more familiar
inhibitors, ketoconazole and erythromycin. Although not studied clinically, these interactions
Significant Inhibitory and Induction Reactions:
may alter the antitumor activity and/or toxicity of
vinblastine.101 Concomitant treatment with
Little is known about pharmacokinetic inter-
actions with chemotherapeutic agents, but it is
nifedipine resulted in a 4-fold increase in
likely that important interactions have not been
vincristine's elimination half-life. Clinical studies
identified. The 3A4 enzyme was important in the
are necessary to validate the pharmacokinetic
data, but greater cytotoxicity could be anticipated.102
epipodophylotoxins, tamoxifen, ifosfamide,
Busulfan is another chemotherapeutic agent
paclitaxel, and vinca alkaloids. Although beyond
that may be metabolized through the 3A4 system.
the scope of this review, it is interesting to note
A study in 13 bone marrow transplant recipients
that 3A4 catalyzes the activation of the prodrug
found an average 20% reduction in busulfan
ifosfamide, raising the possibility that it could be
clearance in patients receiving itraconazole
activated in tumor tissues containing this enzyme.
compared with those receiving either fluconazole
Cytochrome 3A4 substrates may also modulate
or placebo. Itraconazole is known to be a more
multidrug resistance to cancer chemotherapy.97
potent inhibitor of 3A4 than fluconazole.34 The
Cyclosporine increased the AUC of doxorubicin
nature of this interaction has yet to be elucidated,
by 55% and decreased doxorubicin clearance by
but inhibition of oxidative metabolism may be a
50%. The addition of cyclosporine also increased
doxorubicin-induced nausea and vomiting.
Similar myelosuppression was observed when
administered concurrently with inducers such
comparing doxorubicin alone with doxorubicin
phenobarbital and phenytoin, with a mean 170%
(60% of the control dose) plus cyclosporine.98
increase in clearance reported with these drugs.
Similar pharmacokinetic results were obtained
On the other hand, concurrent administration
and a higher frequency of drug-related toxicity
with cyclosporine resulted in an 80% increase in
was observed in patients receiving cyclosporine.99
AUC and a 2-fold increase in etoposide half-life.97
Simultaneous administration of doxorubicin and
In vitro, tamoxifen metabolism is inhibited by
paclitaxel also resulted in significantly elevated
erythromycin, cyclosporine, nifedipine, and
concentrations of doxorubicin, suggesting that
diltiazem. No clinical data are available, but
paclitaxel may inhibit its metabolism.100
interactions are likely to occur and should be
Ifosfamide is an alkylating agent that requires
biotransformation to produce its pharmacologically
active cytoxic compound. This activation by the
3A4 system also results in the formation of a
chemotherapeutic agents. However, significant
interactions with cytochrome 3A4 inhibitors or
metabolite by N-dechlorethylation. Few studies
inducers are likely to become more apparent in
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 3. Cytochrome 2D6 Isoenzyme: Substrates, Inducers, and Inhibitors2, 3, 9, 16, 19, 33, 43, 48, 58, 60, 70, 96, 114, 120–125 Substrates
Significant Inhibitory Interactions: Protease
interactions with these agents, but the potential
for interactions has been addressed based onpharmacokinetic in vitro data.108 The majority of
As previously described, protease inhibitors
these data are with ritonavir, but prescribers
saquinavir, ritonavir, indinavir, and nelfinavir are
should be aware that concomitant administration
substrates and inhibitors of the cytochrome 3A4
of drugs metabolized by the 3A4 system with
system. Ritonavir is also a significant inhibitor of
other protease inhibitors may also result in
the 2D6 isoenzyme system (Table 3).2, 3, 9, 16, 19, 33,
inhibitor ketoconazole with indinavir should
combination with nucleosides and several other
include a dosage reduction of indinavir to 600
drugs (e.g., antimicrobials, antivirals) used to
mg every 8 hours.62 Ketoconazole increases the
treat infections in patients with the acquired
AUC of saquinavir by 150%, but the consistency
immunodeficiency syndrome. When comparing
and extent of this interaction varies widely
these agents, ritonavir appears to be a more
among patients.125 Generally, when given in
potent inhibitor, and patients receiving it will
combination with saquinavir, dosage adjustment
require additional monitoring to avoid significant
is not required unless ketoconazole dosages
interactions. Indinavir appears to less potent and
is a reversible inhibitor of 3A4.125 Therefore, it
Fluconazole's effect on protease inhibitor
may be rational to give ritonavir in the early stage
concentrations is unknown, but it may not
of human immunodeficiency virus (HIV) disease
before a patient begins receiving numerous drugs
concentrations as the addition of ketoconazole
that may interact and require complex dosage
because it is not thought to be as potent of an
inhibitor.125 Similarly, concomitant administration
Due to the poor absorption of saquinavir, it has
of fluconazole 200 mg/day and ritonavir 200 mg
been studied in combination with ritonavir to
4 times/day resulted in insignificant changes in
increase its plasma concentrations. Ritonavir has
the half-life of ritonavir. Dosage adjustments are
increased saquinavir concentrations by 18-fold.125
This concept of combination therapy with other
protease inhibitors warrants further study.
concentrations by inhibiting 3A4 metabolism.
Occupational exposure to HIV may now result
Ritonavir and nelfinavir increase the rifabutin
in a 4-week course of indinavir or other protease
AUC by 4-fold and 207%, respectively.63–65 These
inhibitor.105 Little clinical information and few
increases are associated with an increased risk of
case reports are available regarding drug
side effects including uveitis, making the
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsTable 4. 2D6 Clinically Significant Drug Interactions2, 3, 9, 16, 19, 33, 38, 43, 48, 58, 60, 70, 96, 114, 120–130
analgesic effects; higher riskin PMs and EMs taking inhibitors;reduced morphine conc by 95%.
in serum conc with QRSprolongation; monitor ECG.
Chronic ETOH ingestion (ind)Acute ETOH ingestion (inh)
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 4. 2D6 Clinically Significant Drug Interactions2, 3, 9, 16, 19, 33, 38, 43, 48, 58, 60, 70, 96, 114, 120–130 (continued)
DesipramineImipramineMaprotilineNortriptyline
haloperidol; monitor for side effects.
PMs = poor metabolizers; EMs = extensive metabolizers; AUC = area under the concentration-time curve; SE = side effects; PAH = polycyclicaromatic hydrocarbons; TCA = tricyclic antidepressant.
combination contraindicated.125 Concomitant
administration of indinavir with rifabutin led to
Benzodiazepines and opiates have demonstrated
a 204% increase in rifabutin AUC. Therefore, an
reduced clearance when given in combination
adjustment to one-half the standard rifabutin
with ritonavir and indinavir. If used in combi-
dosage is recommended for patients receiving
nation with protease inhibitors, dosages should
this combination.62, 125 Of note, a similar
be reduced or alternative agents should be
interaction was observed between rifabutin and
fluconazole, making monitoring for ocular side
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
ritonavir and noted to have a significant (> 3-fold)
Table 5. Cytochrome 1A2 Isoenzyme: Substrates,
increase in their AUC include benzodiazepines,
Inducers, and Inhibitors2, 3, 9, 16, 18, 36, 37, 39, 40, 45, 96, 114, 117, 120, 131–139
calcium channel blockers, antidepressants,antiarrhythmics, corticosteroids, anticoagulants,
and opiates.125 Ritonavir increased the AUC of
many 2D6-metabolized drugs by 1.5- to 3-fold
(Table 4),2, 3, 9, 16, 19, 33, 43, 48, 58, 60, 70, 114, 120–130 together
with changes in some 1A2-metabolized drugs
(Table 5).2, 3, 9, 16, 18, 36, 37, 39, 40, 45, 96, 114, 117, 120, 131–139
Large dosage adjustments (50% reduction) may
Ritonavir caused a 77% increase in the AUC of
clarithromycin. Prescribing information for
ritonavir recommends no dosage adjustment in
patients with normal renal function, a 50%
reduction in clarithromycin dosage in patients
with creatinine clearance (Clcr) of 30–60
ml/minute, and a 75% reduction for Clcr below
30 ml/minute. Another specific example of an
AUC increase associated with ritonavir is
PAH = polycyclic aromatic hydrocarbons.
Desipramine dosages should be decreased whenthe drug is given concurrently with ritonavir.60
cautiously in combination with drugs primarily
discontinued during rifampin therapy, two
options are available. The first is to administer a
metabolized by the 2D6 system (ritonavir only).
four-drug tuberculosis regimen that includes
rifampin for a minimum of 2 months or until
accompanied by careful clinical monitoring for
side effects and dosage adjustments is some
achieved. Rifampin can be discontinued and a
modified regimen continued for 16 additionalmonths after that time. This option cannot be
Significant Induction Interactions: Protease
attempted in isoniazid-resistant patients. Option
2 is to continue protease inhibitor therapy withindinavir 800 mg every 8 hours, or switch to
One major interaction of concern with these
indinavir if the patient is taking another protease
drugs is rifampin's and rifabutin's induction of
inhibitor, and administer a four-drug, 9-month
metabolism. Rifampin 300–600 mg/day decreased
regimen that contains rifabutin 150 mg/day (one-
half usual dosage) instead of rifampin. This is
saquinavir dosage adjustments necessary.
based on the fact that rifabutin has less inducing
Rifampin decreased the maximum concentration
respectively.125 Rifabutin is a less potent inducer
Other agents that are known inducers of 3A4,
than rifampin, but decreased saquinavir plasma
including phenobarbital, phenytoin, carbamazepine,
concentrations by 40%.61, 125 The clinical
and dexamethasone, should be given cautiously
significance of these decreases in protease
with these drugs; alternatives are recommended,
inhibitor concentrations is unknown, but given
if possible.125 Tobacco, another known inducer,
the fact that resistance is associated with
is associated with an 18% decrease in the AUC of
ritonavir.60 Specific dosage adjustments in
Guidelines for concomitant administration of
rifampin with protease inhibitors were published
recently by the Centers for Disease Control andPrevention in the Morbidity and Mortality Weekly
Numerous drug interactions with cyclosporine
Report.59 If protease inhibitor therapy cannot be
have surfaced in recent years that are associated
PHARMACOTHERAPY Volume 18, Number 1, 1998
with its metabolism and presystemic metabolism
a higher-dose oral contraceptive (50 µg ethinyl
by the 3A4 enzyme in the liver and intestine,
estradiol), medroxyprogesterone, or nonhormonal
respectively. It is postulated that gastrointestinal
alternative method of contraception is desirable.
tract metabolism may in part explain its erratic
Similarly, corticosteroid clearance is increased
absorption.107–109 In fact, 3A4 inhibition has been
with the same concomitant agents. Patients
given intentionally to improve cyclosporine's
receiving corticosteroids for chronic diseases
requirements. Ketoconazole 200–400 mg/day
can decrease dosage requirements by 60–80%.
Serum concentrations begin to increase within 2
benzodiazepines, which also may compete with
days, but 2–4 weeks may be required for
or induce microsomal hepatic enzymes. They
may reduce the effectiveness of oral contraceptives,
whereas oral contraceptives can enhance the
cyclosporine dosage requirements by as much as
effect of benzodiazepines by competing with
30%.112 In some studies, grapefruit juice
increased the drug's AUC by 19–60% when given
benzodiazepines, an alternative method of
within 90 minutes before or after cyclosporine.52,
contraception is desirable. Oral contraceptives
However, other authors showed no change in
themselves reduce prednisolone clearance up to
cyclosporine AUC or trough concentrations with
50%, increase serum phenytoin concentrations,
concomitant administration of grapefruit juice
decrease metoprolol clearance, and reduce
1.5 L/day.55 Therefore, the effect with grapefruit
juice is highly variable, and the clinical
clinically significant these interactions are
A study in pediatric renal transplant recipients
showed that lower dosages of cyclosporine are
Significant Inhibitory Interactions: Corticosteroids
required in patients also receiving norfloxacin.
Little information is available regarding
This has not been seen with ciprofloxacin.113
inhibition of estrogen or corticosteroid metabolism.
Other drugs that alter cyclosporine concen-
trations secondary to cytochrome 3A4 inhibition
prednisolone and methylprednisolone in humans
include verapamil, nicardipine,107–109 fluconazole,
through inhibition of metabolism. Further
itraconazole, ketoconazole, erythromycin,
studies are required to clarify the clinical
clarithromycin,33, 108, 109 tacrolimus,108, 109 and
mibefradil.38 Cyclosporine concentrations aredecreased secondary to enzyme induction with
2D6 Isoenzyme
rifampin,16, 33, 108, 109, 114 phenytoin, carbamazepine,and phenobarbital.108, 109,120 Cyclosporine trough
identified over 15 years ago. Administration of
discontinued in combination with cyclosporine.
dextromethorphan followed by measurement ofO-demethylated metabolite excretion in urine is
Significant Induction Interactions: Estrogens and
an accurate and noninvasive way of phenotyping
individuals as either EMs or PMs for 2D6 activity. The PMs lack this enzyme as a result of an
autosomal recessively transmitted defect in its
unintended pregnancies due to drug interactions
expression. Of note, approximately 5–10% of
are increasing, perhaps due to the fact that estrogen
whites are PMs compared with 1–3% of African-
and progestin concentrations of oral contraceptives
are decreased. Clinically significant drug
interactions with oral contraceptives secondary
clearance to an inactive metabolite by 2D6, PMs
to 3A4 enzyme induction include carbamazepine,
may have a larger response and be at greater risk
of toxicity than EMs. For example, there is an
primidone, and rifampin,114, 115, 117, 120 They have
not been reported with gabapentin, lamotrigine,
antidepressant-induced cardiotoxicity and with
topiramate, and valproate. With these interactions,
neuroleptic-induced side effects.19 Furthermore,
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
inhibition can reduce the metabolic rate in an
warranted (Table 4).2, 3, 9, 16, 19, 33, 38, 43, 48, 58, 60, 70, 114,
EM to a value comparable with that of a PM.2, 5, 9,
trazodone, with serotonergic syndrome occurring
metabolite by 2D6 (e.g., conversion of codeine to
with 24 hours of administration of paroxetine 20
morphine), the drug may be ineffective in PMs.
Induction cannot convert PMs to EMs, because
We encountered a potential drug interaction in
only inactive or relatively inactive forms of the
our institution that may have been mediated
partly by fluoxetine inhibition of the 2D6 system.
A 59-year-old woman was admitted for Achilles
identified,21, 9 but significant interactions between
tendon repair. Her baseline QT interval on
2D6-metabolized drugs with the well-known
admission was prolonged (497 msec). Her drugs
inducers rifampin114 and anticonvulsants120 have
before admission included cyclobenzaprine,
Large numbers of drugs affecting the cardio-
triamterene-hydrochlorothiazide. She had no
vascular and central nervous systems have been
known history of cardiac disorders except for
identified as substrates for 2D6 (Table 3).2, 9, 39, 40,
hypertension. During outpatient surgery she had
sudden onset of torsades de pointes thatdeteriorated into ventricular fibrillation.
Preoperatively, she received droperidol, which is
known to potentiate QT prolongation and shouldbe given cautiously to patients with baseline QT
In vivo, the selective serotonin reuptake
inhibitor (SSRI) antidepressants fluoxetine and
normal sinus rhythm with magnesium sulfate
paroxetine are equipotent inhibitors of 2D6.
and defibrillation. All drugs were discontinued,
Sertraline has less pronounced inhibition, and
and her QT interval returned to below baseline
fluvoxamine is almost devoid of inhibitory
levels by postoperative day 1. The question
effects.9, 122, 132 Coadministration with tricyclic
remained about the etiology of her baseline QT
antidepressants (TCAs) has been a focus of
prolongation; we postulated inhibition of
interest since these drugs are coadministered in
cyclobenzaprine metabolism by fluoxetine.
some cases for resistant patients. Administration
Cyclobenzaprine is hepatically metabolized,
of desipramine with fluoxetine 20 mg/day and
has a structure similar to TCAs (2D6, 3A4, 1A2
paroxetine 20 mg/day produced up to 4-and 3-
metabolized),96 and caused conduction abnormalities
fold increases, respectively, in peak serum
in cases of overdose. In addition, its average half-
concentrations. Similar results were shown with
life is 24 hours, which corresponds to the gradual
nortriptyline and imipramine.9 This inhibition
decrease in the patient’s QT interval.127 Fluoxetine
is reversed within 1 week of discontinuing
is a known inhibitor of 2D6, 3A4, and 2C, and
paroxetine, 1–2 weeks with sertraline, and up to
reportedly increases serum concentrations of
5 weeks with fluoxetine because of the prolonged
TCAs due to these effects.9, 19, 122–124 Although not
half-lives of the parent compound and its
documented, the potential exists for inhibition of
cyclobenzaprine metabolism by fluoxetine.
On average, the percentage increase in TCA
Interactions secondary to enzyme inhibition by
plasma concentrations over baseline has ranged
SSRIs and that are documented by pharmaco-
from 58–150% with sertraline 50 mg/day and
kinetic studies and case reports occurred with
110–375% with fluoxetine 20 mg/day.19 Clinical
flecainide, propafenone, haloperidol, and other
sequelae resulting from the coadministration of
antipsychotics. Due to the narrow therapeutic
SSRIs and TCAs have been reported only rarely,
index and high-risk patients who receive type Ic
but full dosages of both agents could clearly lead
antiarrhythmics, SSRIs should be avoided in
to plasma concentrations in the toxic range. A
patients taking these drugs.19 Vigilant pharmaco-
summary of 25 cases involving combinations of
dynamic monitoring should accompany therapy
fluoxetine and various TCAs showed that the
with SSRIs in patients treated with other drugs
magnitude of increased TCA concentrations is
variable, does not correlate with the occurrence
of adverse effects, and is not predictable.124
identified as a 2D6 substrate or inhibitor, a report
Lower dosages with these combinations along
with careful monitoring for side effects seem
receiving long-term fluoxetine 80 mg/day and
PHARMACOTHERAPY Volume 18, Number 1, 1998
clarithromycin indicates this potential. The
effect is achievable. Codeine is a prodrug and
patient’s delirium quickly cleared after he stopped
10% of the dose is O-demethylated to the active
the drugs, and did not recur with erythromycin
metabolite, morphine. This demethylation is
alone or when he restarted fluoxetine 80 mg/day.
impaired in PMs and reduced in EMs during
The authors concluded that the delirium was
treatment with inhibitor drugs.3 The combination
consistent with fluoxetine intoxication, which
should probably be avoided since diminution of
codeine’s effect is is highly probable.
Other potential interactions with TCAs include
1A2 Isoenzyme
mibefradil and quinidine. Quinidine is the mostpotent 2D6 inhibitor identified to date.39 It
The 1A2 isoenzyme is of clinical interest
inhibited TCA metabolism and resulted in 85%
because of the large number of drug interactions
reduction in desipramine clearance and a 35%
associated with theophylline dealkylation and
decrease in imipramine clearance.129 Mibefradil
because of its inducibility by PAH in cigarette
is a CYP2D6 inhibitor and can increase plasma
smoke and charcoal-broiled foods. No genetic
levels of TCAs, necessitating substantial dosage
polymorphism has been defined but possibly
reductions.38 Patients receiving these combinations
exists because of observations of a trimodal
should be monitored for signs of TCA toxicity.
pattern of caffeine metabolism. The 1A2 enzymeis also responsible for metabolism of the R-
Significant Induction Interactions: Narcotic
isomer of warfarin as well as with severalbenzodiazepines. As noted in Table 5,2, 3, 9, 16, 18, 36,
37, 39, 40, 45, 96, 114, 117, 120, 131–139 drugs known to be
inhibitors of 1A2 include fluvoxamine (very
methadone, and morphine are metabolized by
potent),2, 19, 39, 132 cimetidine,13, 131 macrolides,36, 37,
131 and several of the quinolones.131,134–136
interactions result from enzyme induction andloss of opioid activity.70 Rifampin 600–900
Significant Inhibitory Interactions: Theophylline
mg/day precipitated withdrawal symptoms whengiven to 21 patients with tuberculosis receiving
Cimetidine is an enzyme inhibitor and causes a
methadone maintenance.130 Similar effects were
pharmacokinetic interaction with theophylline
(theophylline clearance is decreased approximately
Consideration should be given to opioid dosage
30%). Pharmacodynamic data are lacking, however.
increases when rifampin is begun, and patients
An initial dosage reduction should be considered
should be monitored closely for symptoms of
in patients with a baseline theophylline level
withdrawal. Similar enzyme-inducing effects and
above 12 µg/ml due to theophylline's narrow
signs of narcotic withdrawal with up to 50%
reduction in methadone concentrations were
Fluvoxamine is a potent inhibitor of 1A2,
unlike the other SSRIs. It increased theophylline
phenobarbital, and carbamazepine. Pharmaco-
concentrations 2- to 3-fold, along with significant
kinetic studies also indicated that reductions in
increases in haloperidol and clozapine concen-
the clearance of meperidine could be expected
trations.19, 132 The majority of patients had
with these enzyme-inducing agents.70, 120
increased plasma theophylline concentrations
Pharmacodynamic monitoring would appear to
be the most appropriate management strategy
Interactions with macrolides are fairly well
when narcotics are given concurrently with
documented. In most studies, erythromycin and
enzyme-inducing agents.2, 3, 9, 16, 19, 33, 43, 48, 58, 60, 70,
clarithromycin decreased theophylline clearance
20–25% after 7 days of concomitant adminis-tration. Most clinicians recommend theophylline
Significant Inhibitory Interactions: Narcotic
dosage reduction and careful monitoring if thebaseline theophylline level is above 12 µg/ml.
Other macrolides such as azithromycin and
Coadministration of cimetidine 1200 mg/day
with meperidine decreased meperidine clearance
alternatives.36, 37,131 In one patient, however,
addition of azithromycin to a maintenance
Special care should be taken when administering
theophylline regimen resulted in an increase in
codeine with 2D6 inhibitors or when no clinical
serum concentration from the usual 12.7–15.5
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
µg/ml to 20 µg/ml, and discontinuation of
several of these drug interactions have been
azithromycin resulted in a 80% decrease in the
concentration. This was confirmed with two
A series of case reports described the inter-
rechallenges.132 Thus, clinicians should be aware
action between warfarin and quinolones that can
of the potential for an interaction with azithromycin.
occur as early as day 2 or as late as day 16 after
Several quinolones commonly decrease theo-
phylline clearance. Enoxacin has the greatest
complications attributed to this interaction have
potential, with a 50–65% reduction in clearance,
been reported as well. Ciprofloxacin, norfloxacin,
followed by ciprofloxacin with a 25–30% decrease
ofloxacin (least likely), nalidixic acid, and
and norfloxacin with a 10–15% decrease.75,
enoxacin were implicated in these reports.
131,134–136 These interactions resulted in symptoms
According to pharmacokinetic studies, the
of theophylline toxicity including seizures. Up to
interaction is probably secondary to inhibition of
the R-stereoisomer of warfarin, which is partly
patients with a baseline theophylline level above
metabolized by the 1A2 isoenzyme.33, 135, 136
12 µg/ml when beginning these combinations.129,
However, several prospective, placebo-controlled
trials showed no clinically significant effect.138, 139
ofloxacin, levofloxacin, lomefloxacin, and spar-
Since warfarin is metabolized by enzymes from
floxacin are unusual, making them alternative
three different families, most individuals may be
able to shunt its metabolism to a noninhibited
Isoniazid also decreases theophylline clearance
pathway. Although this interaction may be rare
after at least 6 days of concomitant administration.
and unpredictable, careful monitoring of the INR
This appears to be most pronounced in slow
is warranted during concomitant therapy (Table
acetylators, with up to a 2-fold increase in theo-
6).2, 3, 9, 16, 18, 36, 37, 39, 40, 45, 114, 117, 120, 131–139 Alternative
quinolones with little to no inhibitory properties
Oral contraceptives decrease theophylline
include levofloxacin, lomefloxacin, and sparfloxacin.
clearance by 30%, necessitating more careful
The manufacturer of fluvoxamine has received
monitoring when starting or discontinuing
11 reports of interactions with warfarin. The
concomitant therapy with theophylline. The
drug increases the measured warfarin concen-
proposed mechanism is inhibition of metabolism.117
trations by 65%; all patients in case reports had
Grapefruit juice has no effect on theophylline
metabolism, although it may have some 1A2
bleeding complications.132 The safety of combining
warfarin with other SSRIs was studied in patientspreviously maintained with warfarin. Fluoxetine
Significant Induction Interactions: Theophylline
appears to have no effect, and both paroxetine
and sertraline caused an increase in prothrombin
enzymes responsible for theophylline metabolism.
time, with reports of minor bleeding with
It was estimated that smokers may require up to
twice the dosage relative to that of nonsmokers,
warranted during therapy with any SSRI.
and a dosage reduction by one-fourth to one-
Warfarin metabolism is known to be inhibited
third during abstinence. Some reports indicate
by cimetidine, but data on pharmacodynamic and
that enzyme induction is present for up to several
clinical effects are lacking. It seems prudent to
monitor the INR carefully during combination
Other well-established induction interactions
therapy or to consider an alternative histamine2
with theophylline including rifampin and the
(H2) antagonist.13 The enzyme-inhibitory effects
anticonvulsant drugs carbamazepine, pheno-
of cimetidine are attributed to its imidazole ring.
barbital, and phenytoin114, 120, 131 are summarizedin Table 6.2, 3, 9, 16, 18, 36, 37, 39, 40, 45, 114, 117, 120, 131–139
Significant Inhibitory Interactions:Antidepressants, Antipsychotics, and
Significant Inhibitory Interactions: R-Warfarin
As discussed, the R-isomer of warfarin is the
Fluvoxamine increases plasma concentrations
with clinical symptoms of toxicity (e.g., confusion,
significant drug interactions have resulted from
tremor, extrapyramidal syndrome) in patients
inhibition of its metabolism. The R-isomer is
receiving amitriptyline (2-fold increase),
partially metabolized by the 3A4 system, and
clomipramine (8-fold), clozapine (3.2- to 11.8-
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 6. 1A2 Clinically Significant Drug Interactions2, 3, 9, 16, 18, 36, 37, 39, 40, 45, 114, 117, 120, 131–139
need initial dosage increase;monitor serum conc.
more careful monitoring ifbaseline level ≥ 12 µg/ml.
increased theophylline dosage maybe required; monitor serum conc.
conc; more pronounced in slowacetylators; monitor serum conc.
significant if > 35 µg estrogen.
monitor serum conc; effects maypersist for 3 mo after smokingcessation.
Fluoxetine (inh)Paroxetine (inh)Sertraline (inh)Zileuton (inh)
CYTOCHROME P-450 DRUG INTERACTIONS MichaletsTable 6. 1A2 Clinically Significant Drug Interactions2, 3, 9, 16, 18, 36, 37, 39, 40, 45, 114, 117, 120, 131–139 (continued)
AUC = area under the concentration-time curve; SC&E = serum concentration and effects; INR = international normalized ratio; PAH =polycyclic aromatic hydrocarbons; EPS = extrapyramidal syndrome.
fold), desipramine (1-fold), and imipramine (1.3-
metabolized by this subfamily.19, 130 In addition,
to 5.7-fold).132 Patients receiving these combi-
as noted in Table 7,2, 13, 65–68, 120, 132, 140–143 chlor-
nations should be monitored for side effects and
amphenicol,33, 120 cimetidine,13, 120 and isoniazid16,
120 are probable inhibitors on the basis ofsignificant interactions with phenytoin.
Significant Induction Interactions:Benzodiazepines
Significant Inhibitory Interactions: Phenytoin
Similar to theophylline, the inducing effects of
Case reports of 26 patients with steady-state
smoking are associated with less drowsiness in
phenytoin concentrations described a 67–309%
patients taking chlordiazepoxide and diazepam.
increase in serum concentrations with the
This was studied in a comprehensive in-hospital
addition of the inhibitor fluoxetine within 5–13
days. Symptoms of toxicity occurred.19 Fluvoxamine,
nonsmokers, light smokers, and heavy smokers
receiving these benzodiazepines. Smokers mayrequire larger dosages of benzodiazepines toachieve a sedative or anxiolytic effect.18
Table 7. Cytochrome 2C Isoenzyme: Substrates, Inducers, and Inhibitors2, 13, 16, 33, 65–68, 120, 132, 140–143 2C Isoenzyme
The 2C subfamily consists of isoenzymes 2C9,
exhibits genetic polymorphism, with 20% of
Asians and African-Americans and 3–5% of
Caucasians reported as PMs.2, 19 Drugs meta-
bolized by the 2C subfamily include phenytoin
(2C9), S-warfarin (2C9), and omeprazole.
Diazepam, clomipramine, amitriptyline, and
imipramine are demethylated by 2C enzymes.
amiodarone (2C9) and omeprazole (2C19).
Fluvoxamine, fluoxetine, and sertraline may
inhibit these enzymes on the basis of increases in
plasma concentrations of drugs believed to be
PHARMACOTHERAPY Volume 18, Number 1, 1998
Table 8. 2C Clinically Significant Drug Interactions2, 11, 13, 15, 16, 19, 33, 65–68, 120, 132, 140–143
carefully when starting andstopping therapy.
carefully; more pronounced inslow acetylators; monitor forataxia, nystagmus, drowsiness.
monitor SC&E; adjust dosagesas necessary.
monitor serum conc carefullyor give alternative.
conc after 14 days; monitor levelscarefully.
within 3–4 weeks; reducedosage based on serum conc.
nausea, vomiting, vertigo; avoidif possible.
decrease dosage 25% whenstarting therapy.
SC&E = serum concentration and effects; INR = international normalized ratio; PT = prothrombin time; SE = side effects.
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
interaction can be seen from 1 week to 2 months
inhibitory effects. The manufacturer has received
after starting amiodarone and may persist 1–3
reports of drug interactions with phenytoin that
weeks after discontinuation. Most clinicians
included nausea, vomiting, and vertigo.132 Due to
recommend reducing the warfarin dosage by 25%
phenytoin's narrow therapeutic window and
when beginning amiodarone therapy.11, 142
nonlinear pharmacokinetics, these combinationsshould be avoided or phenytoin dosages reduced
Significant Induction Interactions: S-Warfarin
(Table 8).2, 11, 13, 15, 16, 19, 33, 65–68, 120, 132, 140–143
Patients previously stabilized with warfarin can
Cases of mild phenytoin intoxication were
suffer failed anticoagulation with the addition of
rifampin, or overanticoagulation when rifampin
cimetidine. Other H2 antagonists are without
is discontinued.16, 114 Similar problems exist with
these effects and would be more desirable
coadministration of carbamazepine, phenobarbital,
choices.13, 120 A study in eight healthy volunteers
showed impaired elimination of phenytoin afteromeprazole 40 mg/day for 8 days. Phenytoin's
Significant Inhibitory Interactions: Benzodiazepines
elimination half-life was increased by an averageof 27%.65 Patients taking these combinations
In vivo, omeprazole inhibits the metabolism of
should be monitored closely, or lansoprazole may
diazepam and increases the elimination half-life
be given as an alternative in patients receiving
of diazepam by an average of 130%. It is not
entirely clear, but the interaction may be 2C9
An increase in phenytoin concentration seems
mediated. Patients receiving this combination
to be predictable when fluconazole is added.
over the long term should be monitored for side
Nystagmus and ataxia occurred in two patients
effects, or alternative agents should be considered.65
with excessive phenytoin concentrations afterinitiation of fluconazole 200–400 mg/day.140
Studies in healthy volunteers showed up to 75%
Our knowledge of and ability to predict drug
increase in AUC and 128% increase in trough
phenytoin concentrations after 14 days of
understanding of substrates, inhibitors, and
inducers of CYP-450 isoenzymes. This review
Isoniazid is another inhibitor that increases
underscores the need for definitive in vivo drug
phenytoin concentrations. This interaction seems
interaction studies and continued patient
to be most pronounced in slow acetylators.16 A
reporting by clinicians, since in vitro data are not
new antiepileptic agent, topiramate, also increases
always consistent with in vivo experience and
phenytoin serum concentrations up to 25% in
since many variables (age, hepatic function,
some patients. Patients should be monitored
multiple metabolic pathways) influence patient
carefully when receiving this combination
outcomes. The information in this review should
help health care providers in making decisions tomanage CYP-450 drug interactions. Clinicians
Significant Induction Interactions: Phenytoin
should be cognizant of potential interactions and
Administration of rifampin with phenytoin and
become familiar with the substrates, inhibitors,
other anticonvulsants can cause therapeutic
and inducers of the common enzymatic pathways
failure due to enzyme induction. Serum concen-
trations should be monitored regularly whenbeginning or discontinuing rifampin with these
Acknowledgments
Special thanks to T. Donald Marsh, Pharm.D.,
FASHP, Director of Pharmacotherapy for the Mountain
Significant Inhibitory Interactions: S-Warfarin
Area Health Education Center and University of NorthCarolina Clinical Associate Professor of Pharmacy for
The S-isomer of warfarin is metabolized by the
editing and advising, and to the pharmacists at
2C9 isoenzyme. A significant interaction that
Mission–St. Joseph’s Health System for their careful
appears to be 2C9 mediated is with amiodarone
and warfarin. Amiodarone decreases the totalbody clearance of both R- and S-warfarin. Any
References
alterations in clearance of the R-isomer could be
1. Brouwer KLR, Dukes GE, Powell JR. Influence of liver
function on drug disposition. In: Evans WE, Schentag JJ,
PHARMACOTHERAPY Volume 18, Number 1, 1998
Jusko WJ, eds. Applied pharmacokinetics. Spokane, WA:
the scalar electrocardiogram: distinguishing a drug effect from
Applied Therapeutics, 1993:6-1–59.
spontaneous variability. Am Heart J 1996;131:472–80.
2. Slaughter RL, Edwards DJ. Recent advances: the cytochrome
25. Woosley RL. Cardiac actions of antihistamines. Annu Rev
P450 enzymes. Ann Pharmacother 1995;29:619–24.
3. Brosen K. Recent developments in hepatic drug oxidation:
26. Francois I, De Nutte N. Nonulcer dyspepsia: effect of the
implications for clinical pharmacokinetics. Clin
gastrointestinal prokinetic drug cisapride. Curr Ther Res
4. Guengerich FP. Catalytic selectivity of human cytochrome
27. Wysowski DK, Bacsanyi J. Cisapride and fatal arrhythmia. N
P450 enzymes: relevance to drug metabolism and toxicity.
28. Inman W, Kubota K. Tachycardia during cisapride treatment.
5. Nebert DW, Adesnich M, Coon MJ, et al. The P450 gene
superfamily: recommended nomenclature. DNA 1987;6:1–11.
29. Bran S, Murray W, Hirsch IB, Plamer JP. Long QT syndrome
6. Coutts RT. Polymorphism in the metabolism of drugs,
during high-dose cisapride. Arch Intern Med 1995;155:765–8.
including antidepressant drugs: comments on phenotyping. J
30. Olsson S, Edwards IR. Tachycardia during cisapride
Psychiatry Neurosci 1994;19:30–44.
7. Kunze KL, Wienkers LC, Thummel KE, Trater WF.
31. Abramowicz M, ed. Fexofenadine. Med Lett 1996;38:95–6.
Warfarin-fluconazole. I. Inhibition of the human cytochrome
32. Kivisto KT, Neuvonen PJ, Klotz U. Inhibition of terfenadine
P450-dependent metabolism of warfarin by fluconazole: in
metabolism: pharmacokinetic and pharmacodynamic
vitro studies. Drug Metab Dispos 1996;24:414–21.
consequences. Clin Pharmacokinet 1994;27:1–5.
8. Black DJ, Kunze KL, Wienkers LC, et al. Warfarin-
33. Gillum JG, Isreal DS, Polk RE. Pharmacokinetic drug
fluconazole. II. A metabolically based drug interaction: in
interactions with antimicrobial agents. Clin Pharmacokinet
vitro studies. Drug Metab Dispos 1996;24:422–8.
9. Ereshefsky L, Riesenman C, Francis Lam YW.
34. Cantilena LR, Sorrels S, Wiley T, Wortham D. Fluconazole
Antidepressant drug interactions and the cytochrome P450
alters terfenadine pharmacokinetics and electrocardiographic
system: the role of cytochrome P450 2D6. Clin Pharmaco-
pharmacodynamics [abstr]. Clin Pharmacol Ther 1995;
10. Cooke CE, Sklar GE, Nappi JM. Possible pharmacokinetic
35. Harris S, Hilligoss DM, Colangelo PM, Eller M, Okerholm R.
interaction with quinidine: ciprofloxacin or metronidazole?
Azithromycin and terfenadine: lack of drug interaction. Clin
11. Heimark LD, Wienkers L, Dunze K, et al. The mechanism of
36. Amsden GW. Macrolides versus azalides: a drug interaction
the interaction between amiodarone and warfarin in humans.
update. Ann Pharmacother 1995;29:906–17.
Clin Pharmacol Ther 1992;51:398–407.
37. van-Rosenteil NA, Adam D. Macrolide antibacterials. Drug
12. Soto J, Alsar MJ, Sacristan JA. Assessment of the time course
interactions of clinical significance. Drug Saf 1995;13:105–22.
of drugs with inhibitory effects of hepatic metabolic activity
38. Abramowicz M, ed. Mibefradil—a new calcium-channel
using successive salivary caffeine tests. Pharmacotherapy
39. DeVane L. Pharmacokinetics of the newer antidepressants:
13. Shinn AF. Clinical relevance of cimetidine drug interactions.
clinical relevance. Am J Med 1994;97(suppl 6A):13S–23.
40. Shen WW. Cytochrome P450 monooxygenases and
14. Pirttiaho HI, Sotaniemi EA, Pelkonen RO, et al. Hepatic
interactions of psychotropic drugs: a five-year update. Int J
blood flow and drug metabolism in patients on enzyme-
inducing anticonvulsants. Eur J Clin Pharmacol
41. Swims MP. Potential terfenadine-fluoxetine interaction. Ann
15. Harder S, Thurmann P. Clinically important drug
42. Marchiando RJ, Cook MD. Probable terfenadine-fluoxetine-
interactions with anticoagulants. an update. Clin
associated cardiac toxicity. Ann Pharmacother 1995;29:
16. Grange JM, Winstanley PA, Davies PDO. Clinically
43. Finley PR. Selective serotonin reuptake inhibitors: pharmaco-
significant drug interactions with antituberculosis agents.
logic profiles and potential therapeutic distinctions. Ann
17. Cupp MJ, Tracy TS. Role of the cytochrome P450 3A
44. Bristol-Myers Squibb Co. Serzone (nefazodone) package
subfamily in drug interactions. US Pharmacist 1997:HS
45. Solvay Pharmaceuticals. Luvox (fluvoxamine) package insert.
18. Schein JR. Cigarette smoking and clinically significant drug
interactions. Ann Pharmacother 1995;29:1139–48.
46. Robinson DS, Roberts DL, Smith JM, et al. The safety profile
19. Nemeroff CB, DeVane L, Pollock BG. Newer antidepressants
of nefazodone. J Clin Psychiatry 1996;57(suppl 2):31–8.
and the cytochrome P450 system. Am J Psychiatry
47. Pfizer, Inc. Zoloft (sertraline) package insert. Wilkes-Barre,
20. Honig PK, Woosley RL, Zamani K, Conner DP, Cantilena
48. Morton WA, Sonne SC, Verga MA. Venlafaxine: a
structurally unique and novel antidepressant. Ann
electrocardiographic pharmacodynamics of terfenadine with
concomitant administration of erythromycin. Clin Pharmacol
49. Kupferschmidt HT, Riem H, Ziegler WH, Meier PJ, Krahenbuhl S. Interaction between grapefruit juice and
21. Mathews DR, McNutt B, Okerholam R, Flicker M, McBride
midazolam in humans. Clin Pharmacol Ther 1995;58:20–8. G. Torsades de pointes occurring in association with
50. Fuhr U, Dummert AL. The fate of naringin in humans: a key
terfenadine use. JAMA 1991;266:2375–6.
to grapefruit juice-drug interactions: Clin Pharmacol Ther
22. Honig PK, Wortham DC, Zamani K, Conner DP, Mullin JC, Cantilena LR. Terfenadine-ketoconazole interaction:
51. Hollander AMJ, van Rooij J, Lentjes EGWM, et al. The effect
pharmacokinetic and electrocardiographic consequences.
of grapefruit juice on cyclosporine and prednisone
metabolism in transplant patients. Clin Pharmacol Ther
23. Monahan BP, Ferguson CL, Killeavy ES, Lloyd BK, Troy J, Cantilena LR. Torsades de pointes occurring in association
52. Spence JD. Drug interactions with grapefruit: whose
with terfenadine use. JAMA 1990;264:2788–90.
responsibility is it to warn the public? Clin Pharmacol Ther
24. Pratt CM, Ruberg S, Morganroth J, et al. Dose-response
relation between terfenadine (Seldane) and the QT interval on
53. Edwards DJ, Bernier SM. Naringin and naringenin are not
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
the primary CYP3A inhibitors in grapefruit juice. Life Sci
78. Backman JT, Olkkola, KT, Neuvonen PJ. Rifampin drastically
reduces plasma concentrations and effects of oral midazolam.
54. Edwards DJ, Bellevue FH, Woster PM. Identification of 6,7-
dihydroxybergamottin, a cytochrome P450 inhibitor, in
79. Villikka K, Kivisto KT, Backman JT, Olkkola KT, Neuvonen
grapefruit juice. Drug Metab Dispos 1996;24:1287–90. PJ. Triazolam is ineffective in patients taking rifampin. Clin
55. Abramowicz M, ed. Grapefruit juice interactions with drugs.
80. Bailey DG, Arnold MO, Strong A, Munoz C, Spence JD.
56. Benton RE, Honig PK, Zamani K, Cantilena LR, Woosley
Effect of grapefruit juice naringin on nisoldipine
RL. Grapefruit juice alters terfenadine pharmacokinetics,
pharmacokinetics. Clin Pharmacol Ther 1993;54:589–94.
resulting in prolongation of repolarization on the
81. Bailey DG, Spence JD, Numoz C, Arnold JMO. Interaction of
electrocardiogram. Clin Pharmacol Ther 1996;59:383–8.
citrus juice with felodipine and nifedipine. Lancet
57. Rau SE, Bend JR, Arnold MO, Tran LT, Spence JD, Bailey DG. Grapefruit juice-terfenadine single-dose interaction:
82. Leidholm H, Nordine G. Erythromycin-felodipine interaction
magnitude, mechanism, and relevance. Clin Pharmacol Ther
[letter]. Drug Intell Clin Pharm 1991;25:1007–8.
83. Bailey DG, Bend JR, Arnold MO, et al. Erythromycin-
58. Anonymous. Hismanal. FDA Med Bull 1996;269(2):4.
felodipine interaction: magnitude, mechanism, and
59. Centers for Disease Control and Prevention. Clinical update:
comparison with grapefruit juice. Clin Pharmacol Ther
impact of HIV protease inhibitors on the treatment of HIV-
infected tuberculosis patients with rifampin. MMWR
84. Neuvonen P, Raimo S. Itraconazole interacts with felodipine.
60. Abbott Laboratories. Norvir (ritonavir) package insert.
85. Tailor S, Gupta A, Walker S, et al. Peripheral edema due to
nifedipine-itraconazole interaction: a case report. Arch
61. Roche Laboratories. Invirase (saquinavir) package insert.
86. Jalava KM, Olkkola KT, Neuvonen PJ. Itraconazole greatly
62. Merck, Sharp & Dohme. Crixivan (indinavir) package insert.
increases plasma concentrations and effects of felodipine. Clin
63. Agouron Pharmaceuticals, Inc. Viracept (nelfinavir) package
87. Bradford RH, Shear CL, Chremos AN, et al. Expanded
clinical evaluation of lovastatin (EXCEL) study results. I.
64. Humphrey PPA. Letter. BMJ 1992;305:1019.
Efficacy in modifying plasma lipoproteins and adverse event
65. Gugler R, Jensen JC. Omeprazole inhibits oxidative drug
profile in 8245 patients with moderate hypercholesterolemia.
metabolism. Studies with diazepam and phenytoin in vivo and
7-ethoxycoumarin in vitro. Gastroenterology 1985;89:
88. Mauro VF. Clinical pharmacokinetics and practical
applications of simvastatin. Clin Pharmacokinet
66. Maton PN. Omeprazole. N Engl J Med 1991;324:965–75.
67. Blum RA. Lansoprazole and omeprazole in the treatment
89. Illingworth DR, Tobert JA. A review of clinical trials
of acid peptic disorders. Am J Health-Syst Pharm 1996;
comparing HMG-CoA reductase inhibitors. Clin Ther
68. Anderson T. Omeprazole drug interaction studies. Clin
90. Neuvonen PJ, Jalava K. Itraconazole drastically increases
plasma concentrations of lovastatin and lovastatin acid. Clin
69. Darlington MR. Hypoprothrombinemia induced by warfarin
sodium and cisapride. Am J Health-Syst Pharm
91. Lees RS, Lees AM.
coadministration of lovastatin and the antifungal agent
70. Maurer PM, Bartkowski RR. Drug interactions of clinical
itraconazole. N Engl J Med 1995;333:664–5.
significance with opioid analgesics. Drug Saf 1993;8:30–48.
92. Ayanian JZ, Ruchs CS, Stone RM. Lovastatin and
71. Kroboth P, Folan M, Lush R, et al. Coadministration of
rhabdomyolysis [letter]. Ann Intern Med 1988;109:682–3.
nefazodone and benzodiazepines. II. Pharmacodynamic
93. Corpier CL, Jones PH, Suke WN, et al. Rhabdomyolysis and
assessment. Abstract presented at the meeting of the
renal injury with lovastatin use. Report of two cases in cardiac
American Society for Clinical Pharmacology and
transplant recipients. JAMA 1988;260:239–41.
Therapeutics, New Orleans, March 30–April 1, 1994.
94. Spach DH, Bauwens JE, Clark CD, et al. Rhabdomyolysis
72. Greene DS, Dockens RC, Salazar DE, Barbhaiya RH.
associated with lovastatin and erythromycin use. West J Med
Coadministration of nefazodone and benzodiazepines. I.
Pharmacokinetic assessment. Abstract presented at the
95. Fromm MF, Busse D, Kroemer HK, Eichelbaum M.
meeting of the American Society for Clinical Pharmacology
Differential induction of prehepatic and hepatic metabolism
and Therapeutics, New Orleans, March 30–April 1, 1994.
of verapamil by rifampin. Hepatology 1996;24:796–801.
73. Barbhaiya RH, Shukla UA, Kroboth PD, Greene DS.
96. Want RW, Liu L, Cheng H. Identification of human liver
Coadministration of nefazodone and benzodiazepines. II. A
cytochrome p450 isoforms involved in the in vitro
pharmacokinetic interaction study with triazolam. J Clin
metabolism of cyclobenzaprine. Drug Metab Dispos
74. Greene DS, Salazar DE, Dockens RC, Kroboth P, Barbhaiya
97. Kivisto KT, Kroemoer HK, Eichelbaum M. The role of RH. Coadministration of nefazodone and benzodiazepines.
human cytochrome P450 enzymes in the metabolism of
III. A pharmacokinetic interaction study with alprazolam. J
anticancer agents: implications for drug interactions. Br J Clin
Clin Psychopharmacol 1995;15:399–408.
75. Lurila H, Olkkola KT, Neuvonen PJ. Lack of interaction of
98. Bartlett NL, Lum BL, Fisher GA, et al. Phase I trial of
erythromycin with temazepam. Ther Drug Monit
doxorubicin with cyclosporine as a modulator of multidrug
resistance. J Clin Oncol 1994;12:835–42.
76. Ahonen J, Olkkola KT, Neuvonen PJ. Lack of effect of
99. Rushing DA, Raber SR, Rodvold KA, Piscitelli SC, Plank GS,
antimycotic itraconazole on the pharmacokinetics or
Tweksbury DA. The effects of cyclosporine on the
pharmacodynamics of temazepam. Ther Drug Monit
pharmacokinetics of doxorubicin in patients with small cell
lung cancer. Cancer 1994;74:834–41.
77. Kharasch ED, Thummel KE. Human alfentanil metabolism by
100. Berg SL, Cowan KH, Balis FM, et al. Pharmacokinetics of
cytochrome P450 3A3/4. An explanation for interindividual
taxol and doxorubicin administered alone and in combination
variability in alfentanil clearance. Anesth Analg
by continuous 72-hour infusion. J Natl Cancer Inst
PHARMACOTHERAPY Volume 18, Number 1, 1998
101. Zhou-Pan XR, Serree E, Zhou XJ, et al. Involvement of
human liver cytochrome P450 3A in vinblastine metabolism:
123. Otton SV, Wu D, Joffe RT, Cheung SW, Sellers EM.
drug interactions. Cancer Res 1993;53:5121–6.
Inhibition by fluoxetine of cytochrome P450 2D6 activity.
102. Fedeli L, Colozza M, Boschette E, et al. Pharmacokinetics of
Clin Pharmacol Ther 1993;53:401–9.
vincristine in cancer patients treated with nifedipine. Cancer
124. Vandel S, Bertschy G, Bonin B, et al. Tricyclic antidepressant
plasma levels after fluoxetine addition. Neuropsychobiology
103. Buggia I, Zecca M, Alessandrino EP, et al. Itraconazole can
increase systemic exposure to busulfan in patients given bone
125. Piscitelli SC, Flexner C, Minor JR, Polis MA, Masur H. Drug
marrow transplantation. Anticancer Res 1996;16:2083–8.
interactions in patients infected with human immuno-
104. Jacolot J, Simon I, Dreano Y, Beaune P, Riche C, Berthou J.
deficiency virus. Clin Infect Dis 1996;23:685–93.
Identification of the cytochrome P450 IIIA family as the
126. Lischke V, Behne M, Doelken P, et al. Droperidol causes a
enzymes involved in the N-demethylation of tamoxifen in
dose-dependent prolongation of the QT interval. Anesth
human liver microsomes. Biochem Pharmacol 1991;41:
127. Merck & Co., Inc. Prescribing information. Flexeril
105. Gerberding JL. Prophylaxis for occupational exposure to
(cyclobenzaprine). West Point, PA; 1996.
HIV. Ann Intern Med 1996;125:497–501.
128. Pollak PT, Sketris IS, MacKenzie SL, Hewlett TJ. Delirium
106. Abramowicz M, ed. New drugs for HIV infection. Med Lett
probably induced by clarithromycin in a patient receiving
fluoxetine. Ann Pharmacother 1995;29:486–8.
107. Liao JS, Reiss WG. Drug-cytokine interactions: focus on
129. Brosen K, Gram LF. Quinidine inhibits the 2-hydroxylation
cyclosporine. Pharmacotherapy 1996;16:401–8.
of imipramine and desipramine but not the demethylation of
108. Yee GC, McGuire TR. Pharmacokinetic drug interactions
imipramine. Eur J Clin Pharmacol 1989;37:155–60.
with cyclosporine. I. Clin Pharmacokinet 1990;19:319–32.
130. Kreek MJ, Garfield JW, Gutjahr CL, Guisi LM. Rifampin-
109. Yee GC, McGuire TR. Pharmacokinetic drug interactions
induced methadone withdrawal. N Engl J Med 1976;294:
with cyclosporine. II. Clin Pharmacokinet 1990;19:400–15.
110. First MR, Schroeder TJ, Michael A, Hariharan S, Weiskittel
131. Upton RA. Pharmacokinetic interactions between P, Alexander JW. Cyclosporine-ketoconazole interactions.
theophylline and other medication. I. Clin Pharmacokinet
Long-term follow-up and preliminary results of a randomized
trial. Transplantation. 1993;55:1000–4.
132. Wagner W, Vause EW. Fluvoxamine: a review of global drug-
111. Gomez DY, Wacher VJ, Tomlanovich SJ, Hebert MF, Benet
drug interactions data. Clin Pharmacokinet 1995;29:26–32. LZ. The effects of ketoconazole on the intestinal metabolism
133. Pollak PT, Slayter KL. Reduced serum theophylline
and bioavailability of cyclosporine. Clin Pharmacol Ther
concentrations after discontinuation of azithromycin:
evidence for an unusual interactions. Pharmacotherapy
112. Shennib H, Auger JL. Diltiazem improves cyclosporine dosage
in cystic fibrosis lung transplant recipients. J Heart Lung
134. Grasela TH, Dreis MW. An evaluation of the quinolone-
theophylline drug interaction using the Food and Drug
113. McLellan RA, Drobitch RK, McLellan H, Acott PD, Crocker
Administration spontaneous reporting system. Arch Intern
JFS, Renton KW. Norfloxacin interferes with cyclosporine
disposition in pediatric patients undergoing renal
135. Borcherding SM, Stevens R, Nichols RA, Corley CR, Self T.
transplantation. Clin Pharmacol Ther 1995;58:322–7.
Quinolones: a practical review of clinical uses, dosing
114. Venkatesan K. Pharmacokinetic drug interactions with
considerations, and drug interactions. J Fam Pract
rifampicin. Clin Pharmacokinet 1992;22:47–65.
115. Bolt HM. Interactions between clinically used drugs and oral
136. Brouwers JR. Drug interactions with quinolone antibacterials.
contraceptives. Environ Health Perspect 1994;102(suppl
137. Fuhr U, Maier A, Keller A, Steinijans VW, Sauter R, Staib
116. Brooks SM, Werk EE, Ackerman SJ, Sullivan I, Thrasher K. AH. Lacking effect of grapefruit juice on theophylline
Adverse effects of phenobarbital on corticosteroid metabolism
pharmacokinetics. Int J Clin Pharmacol Ther
in patients with bronchial asthma. N Engl J Med 1972;286:
138. Bianco TM, Bussey HI, Farnett LE, et al. Potential warfarin-
117. Dickey RM, ed. Managing contraceptive pill patients, 8th ed.
ciprofloxacin interaction in patients receiving long-term
anticoagulation. Pharmacotherapy 1992;12:435–9.
118. Abramowicz M, ed. Terbinafine for onychomycosis. Med Lett
139. Toon S, Hopkins KJ, Garstang FM, Arrons L, Sedman A, Rowland M. Enoxacin-warfarin interaction: pharmacokinetic
119. Oberg K, Bauman JL. QT interval prolongation and torsades
and stereochemical aspects. Clin Pharmacol Ther 1987;42:
de pointes due to erythromycin lactobionate.
140. Mitchell AS, Holland JT. Fluconazole and phenytoin: a
120. Levy RH. Cytochrome P450 isoenzyme and antiepileptic drug
predictable interactions. Br Med J 1989;298:1315.
interactions. Epilepsia 1995;36(suppl 5):S8–13.
141. Ortho Pharmaceutical Corporation. Topamax (topiramate)
121. Fischer V, Vogels B, Maurer G, Tynes RE. The antipsychotic
clozapine is metabolized by the polymorphic human
142. Harder S, Thurmann P. Clinically important drug
microsomal and recombinant cytochrome P450 2D6. J
interactions with anticoagulants. An update. Clin Pharmaco-
Pharmacol Exp Ther 1992;260:1355–60.
122. Brosen K. Are pharmacokinetic drug interactions with the
143. Landes BD, Petite JP, Flouvat B. Clinical pharmacokinetics of
SSRIs an issue? Int Clin Psychopharmacol 1996;11(suppl
lansoprazole. Clin Pharmacokinet 1995;28:458–70.
UNIVERSIDAD NACIONAL AUTÓNOMA DE NICARAGUA UNAN-MANAGUA VICE RECTORÍA ACADÉMICA “ AÑO DE LA TRANSFORMACIÓN CURRICULAR ” CALENDARIO ACADÉMICO 2011 CURSOS REGULARES CURSOS SABATINOS (PROFESIONALIZACIÓNY POR ENCUENTROS) PRIMER INGRESO 2011 CURSOS DE VERANO 2011 ACTIVIDADES ESPECIALES VACACIONES DEL PERSONAL FERIADOS NACIONALES Y LOCALES
What is Text? Content-based Structure ATHENS, Greece (Ap) A strong earthquake shook theAegean Sea island of Crete on Sunday but caused no in-• Describe the strength and the impact of anjuries or damage. The quake had a preliminary magni-tude of 5.2 and occurred at 5:28 am (0328 GMT) on thesea floor 70 kilometers (44 miles) south of the Cretanport of Chania. The Athens seismological ins
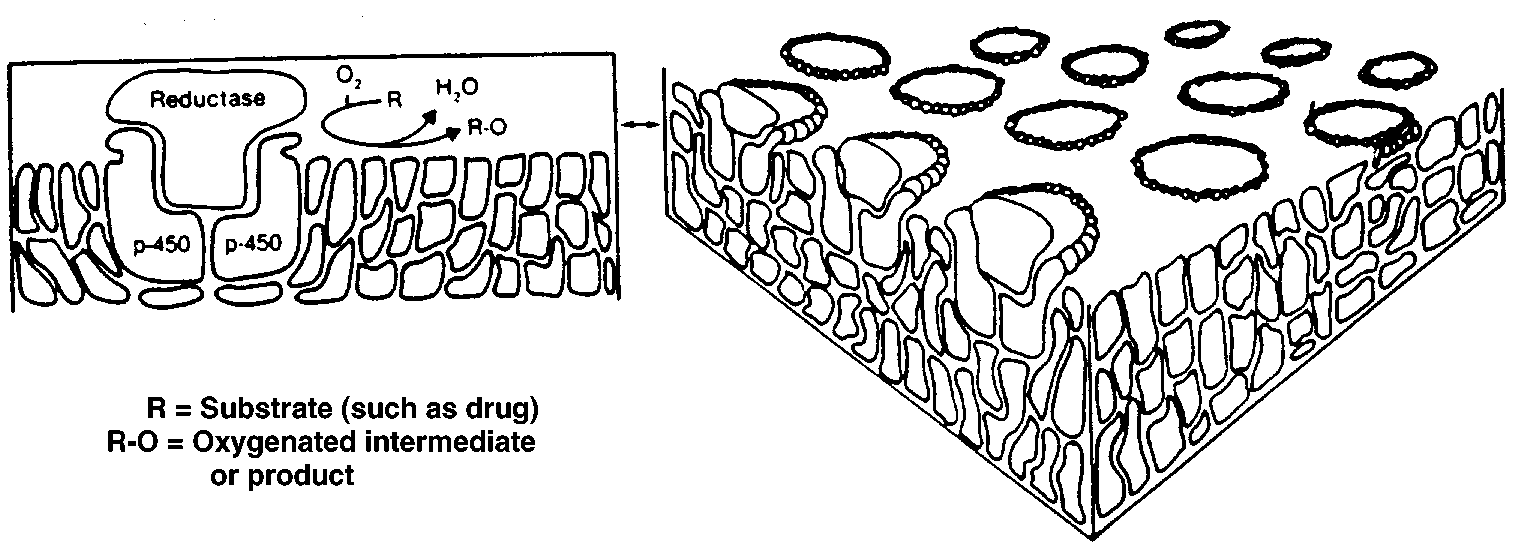 CYTOCHROME P-450 DRUG INTERACTIONS Michalets
Nomenclature
CYTOCHROME P-450 DRUG INTERACTIONS Michalets
Nomenclature