Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Cddlasmercedes.com
Prognostic significance of ischemicelectrocardiographic changes during vasodilatorstress testing in patients with normal SPECT images
Elizabeth Klodas, MD,a Todd D. Miller, MD,a Timothy F. Christian, MD,a David O. Hodge, MS,b and Raymond J. Gibbons, MDa
Background. Patients with ischemic electrocardiographic (ECG) findings during exercise stress testing but normal perfusion images generally have a low risk of cardiac death or myocardial infarction (<1% per year). During vasodilator stress testing, however, the prog- nostic significance of the combination of normal perfusion images and ischemic ECG changes is unknown. Methods and Results. Among 5526 patients who underwent vasodilator stress single photon emission computed tomography (SPECT), 49 (0.9%) had normal images but ischemic ECG changes. A unique feature of this population was that 43 (88%) were women with a mean age of 67 ؎ 10 years. Ischemic ECG changes occurred at a mean heart rate of 101 ؎ 15 beats per minute and persisted for 6.8 ؎ 4.7 minutes after termination of drug infusion. During follow-up of 28 ؎ 20 months, cardiac death occurred in 2 patients and nonfatal myocardial infarction in 4 patients. The rate of cardiac death or nonfatal myocardial infarction was 4% at 1 year, 10% at 2 years, and 14% at 3 years. Of the 12 patients who underwent coronary angiography or autopsy during follow-up, 11 had multivessel coronary artery disease, indicating that these patients likely had false-negative SPECT image results. Eight patients required coronary revascularization. Conclusions. The finding of ischemic ECG changes with normal SPECT images during vasodilator infusion is uncommon, occurs primarily in older women, and is associated with a higher subsequent cardiac event rate than is customarily associated with normal images. (J Nucl Cardiol 2003;10:4-8.) Key Words: Vasodilator stress • single photon emission • computed tomography • electrocardiography • prognosis
modestly worse prognosis (annual risk of cardiac death
See related article, p. 87
or myocardial infarction of 1.3%-2.3%).IschemicECG changes during adenosine or dipyridamole infusion
Patients with normal exercise single photon emis-
occur less commonly than during exercise but when
sion computed tomography (SPECT) images generally
present are predictive of 3-vessel or left main coronary
have an excellent prognosis (annual risk of cardiac death
artery disease (CAD) and/or worse prognosis.
or myocardial infarction Ͻ1%),even in the presence
Perfusion images in such patients are usually abnormal,
of ischemic electrocardiographic (ECG) changes.Pa-
confirming the presence of CAD.The prognostic
tients with normal vasodilator SPECT images have a
significance of ischemic ECG changes during vasodilatorinfusion and normal SPECT images is unknown. This
From the Divisions Cardiovascular Diseasesa, and Biostatistics,b Mayo
study evaluates the prevalence and prognostic signifi-
Clinic and Foundation, Rochester, Minn. Dr Klodas is currently
cance of ischemic ECG changes and normal SPECT
affiliated with the Center for Diagnostic Imaging, St Louis Park,Minn.
images during vasodilator stress testing.
No external funding was used to perform this study. Received for publication Dec 10, 2001; final revision accepted June 18,
Reprint requests: Todd D. Miller, MD, Mayo Clinic, 200 First St SW,
Patients
Gonda 5, Rochester, MN 55905; [email protected].
Between December 1986 and December 1993, 5526
Copyright 2003 by the American Society of Nuclear Cardiology. 1071-3581/2003/$30.00
patients underwent dipyridamole or adenosine thallium 201 or
technetium 99m sestamibi SPECT in the nuclear cardiology
Ischemic electrocardiography with normal SPECT images
laboratory at the Mayo Clinic, Rochester, Minn. Of these, 49
Table 1. Patient characteristics (n ϭ 49)
patients (0.9%) who had ischemic ECG changes with normalSPECT images formed the study group. Exclusion criteria
Variable
included digitalis use, an electrocardiogram showing pacing orleft bundle branch block, or SPECT images with mild fixed
defects (thought to represent attenuation). Angina was graded
according to the criteria of Diamond.Pretest probability of
CAD was estimated with the use of published tables.The
resting electrocardiogram was coded as normal or abnormal.
Among the 5526 patients, 1440 had a normal resting electro-
Vasodilator Stress Testing
The methods for vasodilator stress testing have been
described previously.Patients were instructed not to con-
sume caffeine for 12 hours before the test. Dipyridamole (n ϭ
25) was infused continuously for 4 minutes at a constant rate of
0.14 mg ⅐ kg–1 ⅐ min–1. Adenosine (n ϭ 24) was infused
continuously for 6 minutes at a constant rate of 140 g ⅐ kg–1
⅐ min–1. Tl-201, 3 to 4 mCi, or Tc-99m sestamibi, 20 to 30 mCi,
was injected intravenously, either 3 to 4 minutes after the
termination of the dipyridamole infusion or at 3 minutes
(midpoint) during the adenosine infusion. ECG rhythm strips
were monitored continuously, and a 12-lead electrocardiogram
was obtained at each minute. The stress electrocardiogram wasinterpreted by the physician or nurse supervising the test. An
*Numbers are percentages unless otherwise stated.
ischemic ECG response was defined as 1.0-mm or greaterhorizontal or downsloping ST-segment depression 80 millisec-onds after the J point compared with baseline. The magnitude
Statistical Analysis
of ST-segment depression was categorized as 1.0 to 1.4 mm,
Estimation of event-free survival was completed with the
1.5 to 1.9 mm, 2.0 to 2.4 mm, and 2.5 mm or greater.
Stress SPECT began 10 to 15 minutes after Tl-201
injection and 30 to 60 minutes after Tc-99m sestamibi injec-tion. Resting Tl-201 studies were acquired 3 to 4 hours after the
stress study. Patients studied after January 1, 1990, underwentreinjection with 1 mCi of Tl-201 before delayed imaging. Characteristics
Patients studied with sestamibi underwent rest imaging on aseparate day. SPECT image processing was performed as
Clinical variables are summarized in Most
previously reported.Stress and rest images were graded by
of the patients were women (88% in the study group vs
consensus of 2 experienced observers using a 24-segment
44% in the overall population referred for testing, P Ͻ
model and a 5-point scale (0, absent uptake; 1, severely
.001) who were postmenopausal and not undergoing
decreased uptake; 2, moderately decreased uptake; 3, mildly
estrogen therapy. Risk factors for CAD and use of
decreased uptake; and 4, normal uptake).
antianginal medications were common. Pretest probabil-ity of CAD was estimated to be low in 16% of patients,intermediate in 55%, and high in 29%. One patient had a
Follow-up
history of myocardial infarction and five patients had ahistory of coronary angioplasty.
Follow-up was performed by chart review or contact by
letter or telephone with patients or their physicians. Significantcardiac events were defined as death, nonfatal myocardial
Rest and Stress Electrocardiograms
infarction, or coronary revascularization. Events were con-firmed by review of hospital records and/or death certificates.
The resting electrocardiogram was normal in 26
Deaths were coded as cardiac or noncardiac by a reviewer
patients (53%) and showed minor ST-T abnormalities in
blinded to other data. The mean follow-up for the study was 28
23 (47%). During stress, 38 patients (78%) had ST-
Ϯ 20 months. Of those patients who were alive at follow-up,
segment depression of 1.0 to 1.4 mm develop, 7 (14%)
78% had follow-up of at least 1 year.
had 1.5 to 1.9 mm, and 4 (8%) had 2.0 mm or greater.
Ischemic electrocardiography with normal SPECT images
(slightly Ͻ1% of patients referred for vasodilatorSPECT) and predominantly affects older women withatypical chest pain. The annual risk of cardiac death ormyocardial infarction in these patients is approximately5%. The general tendency with discrepant ECG andSPECT findings is to rely primarily on the image resultsand to consider the ECG findings as likely representing afalse-positive result. In this particular subset of patients,however, the electrocardiogram appears to identify somehigh-risk patients who escape detection by SPECT. Prior Studies
Patients with normal exercise perfusion scans, in-
Figure 1. Kaplan-Meier plot of survival free of cardiac death or
cluding those with a positive exercise electrocardiogram,
myocardial infarction. The risk of cardiac death or nonfatalmyocardial infarction was 4% at 1 year, 10% at 2 years, and
have an annual risk of cardiac death or myocardial
14% at 3 years. Thinner lines indicate 95% confidence inter-
infarction of less than 1%.In patients with normal
vasodilator images, the annual rate is still low butslightly higher, at 1.3% to 2.3%.None of thesestudies analyzed prognosis in the specific subset of
These ECG changes occurred at a heart rate of 101 Ϯ 15
patients with ischemic ECG changes and normal images.
beats per minute and persisted for 6.8 Ϯ 4.7 minutes after
We did not collect follow-up data on the entire group of
5526 patients who underwent vasodilator SPECT be-tween 1986 and 1993 from whom the study group wasidentified. In a previous study,we identified 225
Follow-up
patients with normal vasodilator SPECT and a normal
Eleven patients had significant cardiac events, in-
electrocardiogram whose annual risk of cardiac death or
cluding 2 cardiac deaths, 4 nonfatal myocardial infarc-
myocardial infarction was 2%, significantly lower than in
tions, and 5 revascularization procedures. One patient
this study’s population of patients with an ischemic
died from malignancy. Of the 11 patients with cardiac
electrocardiogram (log-rank statistic, P ϭ .02). The
events, 9 were women. The annual rate of cardiac death
significance of ST-segment changes during pharmaco-
or myocardial infarction was approximately 5%
logic stress is controversial. Ischemic ECG changes were
, and the annual rate of any cardiac event was 9%
associated with angiographic 3-vessel and/or left main
There were no differences in event rates for
patients undergoing dipyridamole versus adenosine
similarly identified patients at higher risk in some prog-
stress (log-rank test, P ϭ .77 for the endpoint cardiac
nostic studiesbut not in others.Analyzing
death or myocardial infarction). The magnitude of ST-
coronary anatomy in patients with ischemic ECG
segment depression (1.0-1.4, 1.5-1.9, and Ն2.0) was
changes and normal images is difficult. Few patients with
modestly worse in patients with events (73%, 9%, and
normal SPECT images are referred for angiography.
18%, respectively) versus those without events (79%,
The only practical method of studying these patients is to
16%, and 5%, respectively) (P ϭ .02). Of the 12 patients
who underwent coronary angiography or autopsy duringfollow-up, 7 had 3-vessel CAD and 4 had 2-vessel CAD,
Potential Explanations for Study Results
consistent with false-negative SPECT studies. Only 1patient had no significant CAD. Of the remaining 36
Balanced hypoperfusion is commonly cited as a
patients, 18 (50%) continued to have the same symp-
reason for normal images in the presence of 3-vessel
CAD. In this study many of the patients with angio-graphic or necroscopic evaluation of their coronaryarteries had 3-vessel disease. Animal models of severe
DISCUSSION
coronary stenoses have shown that vasodilators canresult in shifts in the endocardial-epicardial flow ratio,
Clinical Importance of Study Results
a finding that conceivably could result in ischemic ECG
The combination of normal images and ischemic
changes but not a perfusion defect. Magnetic resonance
ECG changes during vasodilator SPECT is uncommon
imaging may be able to more accurately address this
Ischemic electrocardiography with normal SPECT images
underwent vasodilator SPECT and coronary angiogra-phy, the magnitude of ST-segment depression was thestrongest among all clinical and stress SPECT variablesfor predicting the high-risk anatomic endpoint of leftmain/3-vessel CAD. Implications
Patients with ischemic ECG changes but normal
SPECT images during vasodilator stress testing are athigher risk than is usually expected for patients withnormal images. Some of these patients probably havenormal coronary arteries and a good prognosis. How-ever, in other patients the ischemic ECG changes appear
Figure 2. Kaplan-Meier plot of survival free of cardiac death, myocardial infarction, or revascularization. The risk of cardiac
to identify patients with prognostically important CAD.
death, nonfatal myocardial infarction, or revascularization was
Coronary angiography should be strongly considered in
11% at 1 year, 19% at 2 years, and 28% at 3 years. Thinner
these patients to resolve the prognostic uncertainty raised
lines indicate 95% confidence intervals.
issue. Another potential but clearly speculative explana-
Acknowledgment
tion is that some patients may have abnormal flowreserve that is manifested as an ECG abnormality but not
We thank Lisa VanDeWalker and Pam McCabe for
as a perfusion defect for unknown reasons. Patients with
secretarial preparation of the manuscript and Tammy Hudson
insignificant CAD and endothelial dysfunction are at
for collection of follow-up data. The authors have indicated
higher risk than patients with normal endothelial func-
they have no financial conflicts of interest.
tion.The preponderance of women in the study groupis not readily explainable. During exercise testing,
References
women are generally thought to be more likely to have afalse-positive ECG result than men. This observation
1. Brown KA. Prognostic value of thallium-201 myocardial perfusion
may relate to both a lower prevalence of disease in
imaging. A diagnostic tool comes of age. [see comments] Circu-
women and the digitalis-like effects of estrogen.The
2. Iskander S, Iskandrian AE. Risk assessment using single-photon
same tendency may apply to pharmacologic stress test-
emission computed tomographic technetium-99m sestamibi imag-
ing. However, the observation that 9 of the 11 cardiac
ing. J Am Coll Cardiol 1998;32:57-62.
events occurred in women indicates that the ischemic
3. Pamelia FX, Gibson RS, Watson DD, Craddock GB, Sirowatka J,
ECG changes in these patients were not simply benign
Beller GA. Prognosis with chest pain and normal thallium-201
exercise scintigrams. Am J Cardiol 1985;55:920-6.
4. Wackers FJT, Russo DJ, Russo D, Clements JP. Prognostic
significance of normal quantitative planar thallium-201 stress
Limitations
scintigraphy in patients with chest pain. J Am Coll Cardiol1985;6:27-30.
The size of the study group was small, and the
5. Raiker K, Sinusas AJ, Wackers FJT, Zaret BL. One-year prognosis
number of events was limited. As a result, the 95%
of patients with normal planar or single-photon emission computedtomographic technetium 99m-labeled sestamibi exercise imaging.
confidence intervals on the survival curves are wide
6. Krishnan R, Lu J, Daw MW, Botvinick EH. Does myocardial
myocardial infarction as low as 1% (the generally ac-
perfusion scintigraphy demonstrate clinical usefulness in patients
cepted rate to categorize a population as low risk) could
with markedly positive exercise tests? An assessment of the
not be excluded with a high degree of certainty. We
method in a high-risk subset. Am Heart J 1994;127:804-16.
7. Gibbons RJ, Hodge DO, Berman DS, Akinboboye OO, Heo J,
believe that this possibility is unlikely. First, the upper
Hachamovitch R, et al. Long-term outcome of patients with
95% confidence interval for survival free of total cardiac
intermediate-risk exercise electrocardiograms who do not have
events including revascularization demonstrated an an-
myocardial perfusion defects on radionuclide imaging. Circulation
nual event rate greater than 3% Revascular-
ization procedures do indicate the presence of significant
8. Hendel RC, Layden JL, Leppo JA. Prognostic value of dipyrid-
amole thallium scintigraphy for evaluation of ischemic heart
CAD. An annual event rate greater than 3% is higher
disease. J Am Coll Cardiol 1990;15:109-16.
than expected in a group of patients with normal SPECT
9. Stratmann HG, Tamesis BR, Younis LT, Wittry MD, Miller DD.
images. Second, in our earlier study of 653 patients who
Prognostic value of dipyridamole technetium-99m sestamibi myo-
Ischemic electrocardiography with normal SPECT images
cardial tomography in patients with stable chest pain who are
24. Christian TF, Miller TD, Bailey KR, Gibbons RJ. Noninvasive
unable to exercise. Am J Cardiol 1994;73:647-52.
identification of severe coronary artery disease using exercise
10. Heller GV, Herman SD, Travin MI, Baron JI, Santos-Ocampo C,
tomographic thallium-201 imaging. Am J Cardiol 1992;70:14-20.
McClellan JR. Independent prognostic value of intravenous dipy-
25. Johnston DL, Daley JR, Hodge DO, Hopfenspirger MR, Gibbons
ridamole with technetium-99m sestamibi tomographic imaging in
RJ. Hemodynamic responses and adverse effects associated with
predicting cardiac events and cardiac-related hospital admissions.
adenosine and dipyridamole pharmacologic stress testing: a com-
parison in 2,000 patients. Mayo Clin Proc 1995;70:331-6.
11. Lette J, Bertrand C, Gossard D, Ruscito O, Cerino M, McNamara
26. Kaplan EL, Meier P. Nonparametric estimation from incomplete
D, et al. Long-term risk stratification with dipyridamole imaging.
observations. J Am Stat Assoc 1958;53:457-81.
27. Virtanen KS, Mattila S, Jarvinen A, Frick MH. Angiographic
12. Hachamovitch R, Berman DS, Kiat H, Cohen I, Lewin HC,
findings in patients exhibiting ischemia after oral dipyridamole. Int
Ammanullah AM, et al. Incremental prognostic value of adenosine
stress myocardial perfusion single-photon emission computed
28. Nishimura S, Mahmarian JJ, Bouce TM. Angiographic and hemo-
tomography and impact on subsequent management in patients
dynamic determinants of myocardial ischemia during adenosine
with or suspected of having myocardial ischemia. Am J Cardiol
thallium-201 scintigraphy in coronary artery disease. Circulation
13. Iskandrian AS, Heo J, Lemlek J, Ogilby JD, Untereker WJ,
29. Leppo JA, O’Brien J, Rothendler JA, Getchell JD, Lee VW.
Iskandrian B, et al. Identification of high risk patients with left
Dipyridamole-thallium-201 scintigraphy in the prediction of future
main and three vessel coronary artery disease by adenosine single
cardiac events after acute myocardial infarction. N Engl J Med
photon emission computed tomographic thallium imaging. Am
30. Boucher CA, Brewster DC, Darling RC, Okada RD, Strauss HW,
14. Hart CY, Miller TD, Hodge DO, Gibbons RJ. Specificity of the
Pohost GM. Determination of cardiac risk by dipyridamole-
stress electrocardiogram during adenosine myocardial perfusion
thallium imaging before peripheral vascular surgery. N Engl J Med
imaging in patients taking digoxin. Am Heart J 2000;140:937-40.
15. Ho KT, Miller TD, Christian TF, Hodge DO, Gibbons RJ.
31. Kamal AM, Fattah AA, Pancholy SB, Aksut S, Cave V, Heo J, et
Prediction of severe coronary artery disease and long-term out-
al. Prognostic value of adenosine single-photon emission com-
come in patients undergoing vasodilator SPECT. J Nucl Cardiol
puted tomographic thallium imaging in medically treated patients
with angiographic evidence of coronary artery disease. J Nucl
16. Hendel RC, Whitfield SS, Villegas BJ, Cutler BS, Leppo JA.
Prediction of late cardiac events by dipyridamole thallium imaging
32. Berman DS, Hachamovitch R, Kiat H, Cohen I, Cabico JA, Wang
in patients undergoing elective vascular surgery. Am J Cardiol
FP, et al. Incremental value of prognostic testing in patients with
known or suspected ischemic heart disease: a basis for optimal
17. Marshall ES, Raichlen JS, Kim SM, Intenzo CM, Sawyer DT,
utilization of exercise technetium-99m sestamibi myocardial per-
Brody EA, et al. Prognostic significance of ST-segment depression
fusion single-photon emission computed tomography [published
during adenosine perfusion imaging. Am Heart J 1995;130:58-66.
erratum appears in J Am Coll Cardiol 1996;27:756]. J Am Coll
18. Chambers CE, Brown KA. Dipyridamole-induced ST segment
depression during thallium-201 imaging in patients with coronary
33. Bateman TM, O’Keefe JHJ, Dong VM, Barnhart C, Ligon RW.
artery disease: angiographic and hemodynamic determinants. J Am
Coronary angiographic rates after stress single-photon emission
computed tomography. J Nucl Cardiol 1995;2:217-23.
19. Villanueva FS, Smith WH, Watson DD, Beller GA. ST-segment
34. Nallamothu N, Pancholy SB, Lee KR, Heo J, Iskandrian AS.
depression during dipyridamole infusion, and its clinical, scinti-
Impact on exercise single-photon emission computed tomographic
graphic and hemodynamic correlates. Am J Cardiol 1992;69:
thallium imaging on patient management and outcome. J Nucl
20. Marshall ES, Raichlen JS, Tighe DA, Paul JJ, Breuninger KM,
35. He ZX, Cwajg E, Hwang W, Hartley CJ, Funk E, Michael LH, et
Chung EK. ST-segment depression during adenosine infusion as a
al. Myocardial blood flow and myocardial uptake of 201-Tl and
predictor of myocardial ischemia. Am Heart J 1994;127:305-11.
99m-Tc-sestamibi during coronary vasodilation induced by CGS-
21. Diamond GA. A clinically relevant classification of chest discom-
21680, a selective adenosine A2A receptor agonist. Circulation
fort. [letter] J Am Coll Cardiol 1983;1(2 Pt 1):574-5.
22. Diamond GA, Forrester JS. Analysis of probability as an aid in the
36. Al Suwaidi JA, Hamasaki S, Higano ST, Nishimura RA, Holmes
clinical diagnosis of coronary artery disease. N Engl J Med
DR Jr, Lerman A. Long-term follow-up of patients with mild
coronary artery disease and endothelial dysfunction. Circulation
23. Gibbons RJ, Zinsmeister AR, Miller TD, Clements IP. Supine
exercise electrocardiography compared with exercise radionuclide
37. Kwok Y, Kim C, Grady D, Segal M, Redberg R. Meta-analysis of
angiography in noninvasive identification of severe coronary artery
exercise testing to detect coronary artery disease in women. Am J
disease [see comments]. Ann Intern Med 1990;112:743-9.
INDIAN JOURNAL OF DENTAL ADVANCEMENTS J o u r n a l h o m e p a g e : w w w. n a c d . i nHarinath Reddy S1, Satyanarayana D2, Vidya Sagar S3, Surykanth M4 Department of Periodontics ABSTRACT: Kamineni Institute of Dental Sciences Chronic inflammatory periodontal disease is caused by host Narketpally, Nalgonda Dist. immune responses to periodontal microorganisms. The past dec
Understanding the Diabetes Medicine Maze Michael Ikeler, M.D. Internal Medicine & Pediatrics Background HbA1c is a test used to measure long-term blood sugar control in people with . Normal HbA1c levels are usually less than 6 percent in people without diabetes; people with diabetes usually have higher HbA1c results. Studies have shown that the higher the HbA1c, the greater the chanc
 Ischemic electrocardiography with normal SPECT images
(slightly Ͻ1% of patients referred for vasodilatorSPECT) and predominantly affects older women withatypical chest pain. The annual risk of cardiac death ormyocardial infarction in these patients is approximately5%. The general tendency with discrepant ECG andSPECT findings is to rely primarily on the image resultsand to consider the ECG findings as likely representing afalse-positive result. In this particular subset of patients,however, the electrocardiogram appears to identify somehigh-risk patients who escape detection by SPECT.
Ischemic electrocardiography with normal SPECT images
(slightly Ͻ1% of patients referred for vasodilatorSPECT) and predominantly affects older women withatypical chest pain. The annual risk of cardiac death ormyocardial infarction in these patients is approximately5%. The general tendency with discrepant ECG andSPECT findings is to rely primarily on the image resultsand to consider the ECG findings as likely representing afalse-positive result. In this particular subset of patients,however, the electrocardiogram appears to identify somehigh-risk patients who escape detection by SPECT.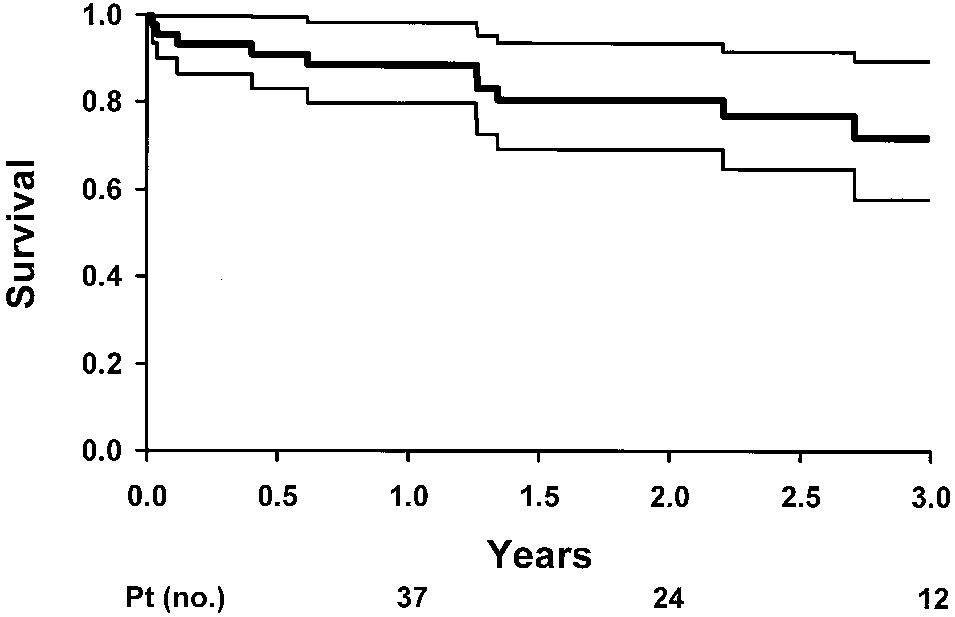 Ischemic electrocardiography with normal SPECT images
underwent vasodilator SPECT and coronary angiogra-phy, the magnitude of ST-segment depression was thestrongest among all clinical and stress SPECT variablesfor predicting the high-risk anatomic endpoint of leftmain/3-vessel CAD.
Ischemic electrocardiography with normal SPECT images
underwent vasodilator SPECT and coronary angiogra-phy, the magnitude of ST-segment depression was thestrongest among all clinical and stress SPECT variablesfor predicting the high-risk anatomic endpoint of leftmain/3-vessel CAD.