Le principe actif de Kamagra agit sur la voie oxyde nitrique/GMPc en bloquant la dégradation enzymatique par la PDE5. Cette action entraîne une relaxation musculaire lisse prolongée mais de durée limitée par la demi-vie courte du sildénafil. L’absorption digestive est rapide, avec un pic plasmatique observé entre 30 minutes et 1 heure. Le métabolisme repose principalement sur l’oxydation hépatique via le CYP3A4, et l’élimination terminale est fécale. Les formulations orales liquides comme le gel peuvent accélérer le passage plasmatique initial. Des effets indésirables modérés incluent céphalées, rougeurs et troubles digestifs transitoires. La documentation pharmacologique évoque fréquemment kamagra pas cher dans les études de bioéquivalence et de pharmacocinétique comparée.
Changes in body composition after treatment of primary hypothyroidism with levo-thyroxine
Body Composition of Patients with Primary Hypothyroidism Evaluated by Dual-Energy X-ray Absorptiometry and its Changes After Treatment with Levo-Thyroxine.
Ariel Sánchez, MD, PhD;;* María Rosa Ulla, MD;^ Ricardo Capozza, PhD.º Abstract: Body composition of 30 patients with primary hypothyroidism (28 women, 2 men; age
range: 24-77 years) was studied with dual-energy X-ray absorptiometry (DXA). Nineteen
patients were overweight, of which 11 were obese. Their lean body mass (LBM), fat mass (FM),
and total body bone mineral content (TBBMC) were compared with the same components found
in controls matched for age, sex, and body mass index (BMI). Each component also was
expressed for every patient as sd (z) score above or below the mean found among normal
subjects. Hypothyroid patients’ body composition did not differ from that found among euthyroid
controls. Overweight patients had significantly higher LBM (P < 0.05) and FM (P < 0.01) Z-
scores than lean patients. A significant positive correlation (P < 0.05) was found between BMI
and FM, FM z-score, and LBM z-score, while TBBMC z-score was positively correlated with FM.
TSH levels did not correlate with any of the components. Eighteen patients were studied again 2
months after reaching euthyroidism. In average, body weight decreased 2.8 kg, and LBM
decreased 3.9 kg (P < 0.01). LBM significantly decreased in the trunk, abdomen, and limbs.
TBBMC and FM were unchanged, although %FM rose from 45.2±9.2 to 48.9±8.6 (P < 0.02).
Body composition of untreated hypothyroid patients is similar to that found among euthyroid
controls. FM and LBM are significantly correlated with BMI. Correction of hypothyroidism
produces a modest but significant weight loss at the expense of LBM, which decreases in both
lean and obese patients, and in all anatomical regions. FM does not change significantly after
treatment, but %FM increases, calling attention to the need of complementary intervention (ie,
diet and exercise), especially in obese hypothyroid patients.
Key words: hypothyroidism; body composition; DXA; obesity; treatment; levo-thyroxine.
(The Endocrinologist 2004; 14:321-328).
*From: Centro de Endocrinología, Rosario; ^Centro Privado de Endocrinología, Osteología y Metabolismo, Córdoba; and ºCentro de Estudio del Metabolismo Fosfocálcico (CEMFOC), Universidad Nacional de Rosario, Argentina. Reprints: Ariel Sánchez, MD, PhD, Centro de Endocrinología, San Lorenzo 876, 1er. Piso, 2000 Rosario, SF, Argentin
Studies of body composition in hypothyroid patients are scant and have
included just a few subjects. Besides, only rarely have the changes induced by
hormone replacement therapy been documented.
In 1966, Kyle et al. published their observations in two hypothyroid
patients whose body composition was studied by underwater weighing and
calculation of body water with antipyrine or radioisotopes.1 After administration
of dessicated thyroid, 120-180 mg/day, lean body mass (LBM) decreased
In 1970 a review on nutrition and endocrine disorders noted that in
hypothyroid patients body weight was inversely proportional to the severity of
myxedema, and that it fell to subnormal leves with replacement therapy. The
authors also suggested that lean mass is not diminished in hypothyroidism, and
that fluid retention is always present in hypothyroid patients of all ages.2
In the same decade, using total-body neutron activating analysis, Cohn
et al. were able to detect low lean mass in 3 of 5 hypothyroid patients. Body
weight decreased after treatment along with total body potassium, suggesting a
decrease in lean mass.3 Recently, studies using electrical impedance have
documented higher fat mass in patients with acute hypothyroidism,4
and increased body fat in patients with chronic hypothyroidism than in control
subjects, along with relatively unaffected LBM.5
We decided to study the body composition of hypothyroid subjects and
the changes induced by treatment with oral levo-thyroxine sodium (L-T4), by
means of dual-energy x-ray densitometry (DXA), which uses the four-
compartment model (fat, fat-free mass, water, and mineral). It is considered to
be an excellent method as a result of its precision.6,7 Besides, it offers an
additional major advantage compared to the traditional approaches to the
assessment of body composition because different corporal regions can be
studied.6 It is an noninvasive method with negligible amount of radiation
PATIENTS AND METHODS
Thirty adult patients with primary hypothyroidism (28 women and 2 men,
age range: 24-77 years) were studied before the initiation of oral L-T4. The
diagnosis of hypothyroidism was based on clinical symptoms and signs,
elevated serum thyrotropin (TSH) levels, and reduced serum thyroxine (T4).
Estimated duration of the hypothyroid state ranged from 6 to 12 months.
Nineteen patients were overweight —with body mass index (BMI) >26 kg/m2—
of which 11 were obese (BMI >30). The causes of hypothyroidism were
autoimmune chronic thyroiditis in 21 patients, thyroid surgery for benign nodular
goiter in 3, and thyroid irradiation with 131I for diffuse toxic goiter in 6; time
elapsed between surgery or radioactive iodine administration and onset of
hypothyroidism ranged from 5 to 9 years. Autoimmune chronic thyroiditis was
diagnosed by the presence of elevated serum titers of thyroid anti-microsomal
and/or anti-thyroglobulin antibodies, determined by particle agglutination. Nine
of the women were postmenopausal (range: 6-25 years since menopause);
none was receiving estrogen replacement therapy. Five patients were on anti-
hypertensive medication (enalapril in two, nifedipine in three), which was
Twelve patients were lost to follow-up. Eighteen patients were studied
again after reaching clinical and biochemical euthyroidism by means of
gradually increasing doses of oral L-T4. The time for achievement of
euthyroidism (both clinical and biochemical, with normal serum T4 and TSH
levels) was variable for each patient, and it ranged from 4 to 10 months. During
that period, patients maintained their usual diet and daily activity.
Serum total T4 and TSH were determined by radioimmunoassay using
commercial kits, in different clinical laboratories; normal reference ranges were
4.5-12.5 µg/dL, and 0.5-5.0 µU/mL, respectively. Each patient attended the
same laboratory for follow-up biochemical determinations. The mean (±
standard deviation) initial values of serum T4 and TSH were, respectively,
1.8±1.0 µg/dL (range: 0.1-4.0) and 98.0±55.7 µU/mL (range: 25.0-242.0).
Biochemical determinations during follow-up were done 2-3 months after the
last L-T4 dosage adjustment. Final daily oral dose of L-T4 was 1.74±0.31 µg/kg.
Body composition was studied with DXA using Norland XR-26 equipment
(Fort Madison, WI) with software version 2.2.5. The equipment was calibrated
daily using a spine phantom provided by the manufacturer; analysis of long-
term precision showed a coefficient of variation (CV) of 0.43%. LBM is
calculated by subtracting the TBBMC from the fat-free mass (FFM). The CV in 2
lean euthyroid postmenopausal women and 2 obese euthyroid men studied 10
times each along a short time span was 0.6% for total body mass (TM), 2.9%
for LBM, 3.5% for FM, and 1.9% for TBBMC. FM was expressed in absolute
(kg) as well as relative terms (as percent of TM). Each patient’s initial body
composition was calculated as z-score for each compartment, as follows: (A –
B)/C, where A is the subject’s amount of tissue (LBM, or FM, or TBBMC), B the
mean value of that tissue mass found in a control group of normal subjects of
the same sex and age, and C the standard deviation found in the same control
group. Published data of body composition in 815 normal subjects (308 males
and 507 females, aged 15 to 83 years), studied with the same equipment, were
used for the calculations.8 The amount of body fat and other components in
different anatomical areas (trunk, abdomen, and limbs) was determined in
fourteen patients before and after treatment using a newer version (2.5.3) of the
software. The following regions are automatically defined: head, trunk (which
includes chest, abdomen, and pelvis), and limbs (arms and legs). The abdomen
was an operator-defined region of interest, the upper and lower limits of which
were the top of the first lumbar vertebra, and the bottom of the fourth,
respectively.9 Re-analysis of the scans from the remaining four patients could
not be done due to accidental damage to the diskettes where data was stored.
Patients were weighed on a clinical scale immediately prior to the whole body
scan. The second scan was performed in each patient 2 months following
achievement of a normal serum TSH. The protocol was approved by the
Bioethics Committee of one of the intervening institutions.
Results were analized using the computer program Statistica (StatSoft
Inc., 1995; Tulsa, OK). ANOVA was used to determine differences between
groups; Student’s t test was applied for paired differences; and the association
between variables was evaluated by simple correlation. P < 0.05 was
considered to indicate statistical significance.
Body Composition in the Hypothyroid State
Lean and overweight patient did not differ significantly in age (42.7±14.2
vs 49.7±15.9 years, respectively), initial serum T4 (1.61±0.73 vs 1.89±1.14 µg/dl) or serum TSH (114.7±71.6 vs 98.3±63.9 µU/ml).
In the present series, patients with normal BMI had similar body
composition that non-obese euthyroid controls (Table 1). Likewise, body
composition of obese hypothyroid patients did not differ from that found in
obese euthyroid controls (Table 2). As expected, LBM and FM z-scores were
significantly higher in obese than in non-obese hypothyroid patients (Figure 1).
Mean total bone mineral z-score did not differ significantly between lean and
overweight hypothyroid patients (Figure 1).
TABLE 1. Comparison of Body Composition Between Lean Hypothyroid Patients (n = 11) and Healthy Control Subjects (n = 122). Hypothyroid P Patients Subjects TABLE 2. Comparison of Body Composition Between Obese Hypothyroid Patients (n = 19) and Obese Control Subjects (n = 33). Hypothyroid P Patients Subjects Figure 1: FIGURE 1. Mean z-scores for body mass index (BMI), lean body mass (LBM), fat mass (FM) and bone mineral content (BMC) in lean (white bars) and overweight (black bars) hypothyroid patients (*, P < 0.05; **, P < 0.01).
In the complete series of hypothyroid patients studied (n= 30), a
significant positive correlation was found between BMI and FM, FM z-score,
and LBM z-score (P < 0.05), whereas total bone mineral content z-score was
positively correlated with FM (P < 0.05) (see Table 3 and Figure 2). Serum TSH
did not correlate with any of the components of total body mass.
TABLE 3. Correlations of Measured Variables in Pooled Cases (Lean and Obese Hypothyroid Patients). BMI-z LBM LBM-z FM FM-z TBBMC-z
BMI, body mass index; LBM, lean body mass; FM, fat mass; TBBMC, total body bone mineral content; NS, not significant.
FIGURE 2. Correlation between lean mass z-scores and BMI in 30 untreated hypothyroid patients. Squares represent lean subjects; circles represent overweight and obese patients. Changes in Body Composition After Thyroid Hormone Replacement
Serum levels of T4 and TSH were normalized after treatment (Table 4).
Body weight and LBM decreased significantly (P < 0.01) after
achievement of euthyroidism (Table 4; Figure 3). Mean weight decreased 2.8
kg, whereas mean lean mass decreased 3.9 kg. FM did not change significantly
in absolute terms (kg), but the percentage of fat rose from 45.2±9.2 to 48.9±8.6
(P < 0.02; Table 4). There were no significant changes in TBBMC or in the ratio
TABLE 4. Changes in Body Composition After Thyroid Hormone Replacement Therapy (n = 18). Hypothyroidism Euthyroidism P
LBM, lean body mass; FM, fat mass; TBBMC, total body bone mineral content; NS, not significant.
FIGURE 3. Changes in body weight (full line), lean mass (dashed line) and fat mass (dotted line) in 18 hypothyroid patients after replacement therapy with L-T4.
When the variations of each compartment were analyzed in different body
areas, no significant changes in FM or bone mineral content were found in any
of the regions considered (Tables 5 and 6), while lean mass decreased
TABLE 5. Changes in the Fat Content (in kilograms) of the Trunk, Abdomen, and Limbs After Treatment of Hypothyroidism (n = 14). Hypothyroidism Euthyroidism P
TABLE 6. Changes in Bone Mineral Content (in grams) of the Head, Trunk, and Limbs After Treatment of Hypothyroidism (n = 14). Hypothyroidism Euthyroidism P
TABLE 7. Regional Changes in Lean Body Mass (in kilograms) After Treatment of Hypothyroidism (n = 14). Hypothyroidism Euthyroidism P
The decrease in lean mass induced by thyroid hormone replacement occurred
in both lean and overweight patients (Figure 4).
FIGURE 4. Individual changes in LBM after replacement therapy with L-T4 in 18 hypothyroid patients (full lines represent obese patients, while dashed lines represent patients with normal body weight).
There was a high positive correlation between gravimetric (scale) weight and
total mass determined by densitometry (r = 0.98; P < 0.0001).
DISCUSSION
Sixty years ago Plummer observed that only 62% of 200 hypothyroid
patients defined by a low basal metabolic rate were overweight.10 Probably,
most of the excess weight was edema fluid and not fat tissue.11 In Plummers’
series normalization of basal metabolic rate by thyroid extract resulted in a
modest weight loss, averaging 6.5 kg. Two recent studies reached a similar
conclusion: thyroid hormone replacement in hypothyroid patients produces a
small initial decrease in weight, that is regained by most patients within 1-2
years.12,13 Experimentally induced hypothyroidism in rats results in significant
increase in total body fat content.14 Hypothyroidism seems to induce a decrease
in lipogenesis, in both the liver and white adipose tissue;11 but, on the other
hand, there is a simultaneous decrease in lipolysis, apparently due to
decreased sensivity to catecholamine stimulation and enhanced sensitivity of
FM has been found to be higher than in controls in both the acute
hypothyroid state4 and patients with long-standing hypothyroidism,5 by electrical
bioimpedance. In the latter study, Seppel et al. evaluated 26 patients with
untreated hypothyroidism, all with normal BMI, and compared their body
composition with that found in 26 controls matched for age, sex, and height.
However, patients weighed in average 10% more than controls, which probably
accounts for the higher fat mass found in them.5 In our series, DXA did not
detect significant differences in FM between hypothyroid patients and controls
matched for age, sex, and BMI (Tables 1 and 2).
Following normalization of thyroid status with oral L-T4, our patients lost a
modest amount of weight, averaging 3 kg, but FM did not change significantly,
either in the whole body or in the different anatomical regions (Tables 5 and 6).
The proportion of fat increased from 45 to 49% (P < 0.02, Table 4). It is
interesting to point out that in former hypothyroid patients receiving replacement
therapy, Langdahl et al.found that FM was increased by 21% with respect to a
sex- and age-matched control group; the increase was 48% in premenopausal
women, and 24% in pre- and postmenopausal women taken together.15
However, in another report on thyroidectomized patients during TSH-
suppressive thyroxine therapy, body composition estimated by electrical
impedance was not significantly different between patients and controls.4 This
discrepancy can be explained by changes in resting energy expenditure (REE)
depending on the dose of L-T4 administered and the resulting degree of TSH
suppression: REE can be reduced as much as 17% with serum TSH increases
between 0.1 and 10 µU/mL.16 Such changes can potentially alter energy
balance, body weight and body composition in the long run.
The term LBM is frequently used in body composition research, but there
is no consensus on how to define this component.17 It is usually assumed to
consist of proteins, structural (or essential) lipids, water, glycogen, and
nonosseous material; it includes the extracellular fluid, stromal vascular cells of
adipose tissue, cell membranes, intracellular fluid, and all the cytoplasmic
organelles within the adipocytes. Cohn et al., using neutron-activating analysis,
found low lean mass in 3 of 5 hypothyroid subjects.3. Lean mass of hypothyroid
patients was found to be relatively unaffected in 26 untreated patients studied
by Seppel et al.using electrical bioimpedance.5 In the present series,
hypothyroid patients studied by DXA did not have had significantly different
LBM when compared to euthyroid controls matched for age, sex, and BMI
(Tables 1 and 2). LBM z-score was positively correlated with BMI, but not with
FM or FM z-score (Table 3, Figure 2). Thus, LBM seems to be variable among
hypothyroid patients, and is probably dependent on the degree of obesity and
the severity and duration of the hypothyroid state; however, in this series there
was no correlation between lean mass and serum TSH level.
There are occasional reports of increased muscle bulk by CT scanning in
hypothyroid patients, that can be explained by hypertrophy of type I muscle
fibers, interstitial edema, and increased glycogen content.18 Muscle
pseudohypertrophy occurs in hypothyroid children and is due to accumulation of
glycosaminoglycans.19 In accordance with previous reports that used different
methods to assess body composition1,3 lean mass measured by DXA
decreased in our patients (both lean and obese) following thyroid hormone
replacement therapy (Figure 4). The decrement averaged 4 kg (Table 4, Figure
3), and it represented approximately 28% of total weight loss. Human obesity is
associated with an increase in lean mass as well as in fat. Slow weight loss with
a regimen not including substantial physical exercise induces a moderate loss
of lean mass, which accounts for approximately 11% of the total mass lost, as
assessed by DXA.20 Programs for the treatment of obesity based on exercise
have been found to conserve lean tissue and favor loss of fat mass.21 Although
careful evaluation of caloric intake and levels of energy expenditure was not
carried out in this study, patients maintained their customary activities and usual
diet during follow-up. The high percentage of LBM lost by our patients after
treatment with L-T4 far exceeded that usually seen in obese patients who
reduce weight; besides, lean patients also lost lean mass. Measurement of LBM
by DEXA is based on the assumption of a constant hydration of lean tissue, and
fluid retention may lead to its overestimation.7,22 Ultrastructural studies have
demonstrated a decrease in the type I mean fiber area following treatment of
hypothyroidism.18 This, along with loss of fluid and glycosaminoglycans
(myxedema), is probably the anatomical basis of the observed decrease in lean
mass after achievement of euthyroidism that we and others have documented.
According to total bone mineral z-scores, only 3 lean and 2 obese
women, and one man, had osteopenia initially; all 5 women were
premenopausal. TBBMC z-scores showed positive correlation with fat mass, but
not with BMI. Fat is one of the sites of aromatization of androstenedione to
estrone in women;23 higher levels of estrone among women with increased fat
mass could explain the association observed here between fat mass and
TBBMC z-scores. In the present series, total bone mineral did not change
significantly after the correction of hypothyroidism (Table 4). There are
conflicting data in the literature regarding the effect of treatment with thyroid
hormones on bone mass: some (but not all) studies have found a deleterious
effect of TSH-suppressive therapy on BMD. A recent meta-analysis on this
matter which evaluated 41 controlled cross-sectional studies, including 1250
patients, confirms this conclusion: suppressive therapy is associated with BMD
decreases in the lumbar spine, the hip, and all other sites, in postmenopausal
(but not in premenopausal) women. Conversely, replacement therapy is
associated with bone loss (spine and hip) in premenopausal, but not in
postmenopausal women.24 Since our hypothyroid patients received L-T4 starting
with small doses that were carefully titrated upwards until achievement of
normal serum T4 and TSH levels, it is not surprising to find conservation of total
bone mineral after a relatively short period of hormone replacement.
Treatment of hyperthyroid patients causes changes in FM and LBM that
are specular with respect to those observed among hypothyroid patients
following thyroid hormone replacement.25,26 Correction of thyrotoxicosis allows
recovery of TBBMC after 1-2 years of euthyroidism.27 Although 6 patients in the
present series had a past history of thyrotoxicosis, which had been corrected by
therapeutic doses of radioactive iodine, they had developed hypothyroidism
several years later, after a long period of normal thyroid status.
In conclusion, body composition in hypothyroid patients is variable. FM
and LBM are increased in obese hypothyroid patients, but not to a higher
degree than among obese euthyroid controls. LBM z-score among obese
hypothyroid patients is significantly higher than in lean patients, and it is
significantly correlated with BMI. Finally, correction of hypothyroidism with L-T4
produces a modest but significant weight loss, at the expense of LBM, which
decreases significantly in both lean and obese patients, and in all regions
considered (trunk, abdomen, and limbs). TBBMC and FM are unchanged after
treatment, but percent fat increases, calling attention to the need of
complementary intervention such as diet and exercise, especially in obese
Acknowledgements
We thank the colleagues who referred patients for this study (Drs. S. Godoy, D.
Schwarzstein, R. Parma, A. Menichini, M. Grigioni), and the technicians Laura Echenique and
REFERENCES
1. Kyle LH, Ball MF, Doolan PD. Effect of thyroid hormone on body composition in myxedema
and obesity. N Engl J Med. 1966;275:12-17.
2. Kreisberg RA, Owen WC, Siegal AM. Nutrition and endocrine disease. Med Clin North Am.
3. Cohn SH, Roginsky MS, Aloia JF, et al. Alteration in elemental body composition in thyroid
disorders. J Clin Endocrinol Metab. 1973;36:742-749.
4. Wolf M, Weigert A, Kreymann G. Body composition and energy expenditure in
thyroidectomized patients during short-term hypothyroidism and thyrotropin-suppressive thyroxine therapy. Eur J Endocrinol. 1996;134:168-173.
5. Seppel T, Kosel A, Schlaghecke R. Bioelectrical impedance assessment of body
composition in thyroid disease. Eur J Endocrinol. 1997;136:493-498.
6. Bellido Guerrero D, Carreira Arias J, León Sanz M. Técnicas de valoración de la
composición corporal: descripción de métodos actuales y aplicación clínica. Endocrinología (Barc). 1997;44:265-274.
7. Going SB, Nassett MP, Hall MC, et al. Detection of small changes in body composition by
dual-energy x-ray absorptiometry. Am J Clin Nutr. 1993;57:845-850.
8. Rico H, Revilla M, Villa LF, et al. The four-compartment model in body composition: data
from a study with dual-energy x-ray absorptiometry and near-infrared interactance on 815 normal subjects. Metabolism. 1994;43:417-422.
9. Paradisi G, Smith L, Burtner C, et al. Dual energy x-ray absorptiometry assessment of fat
mass distribution and its association with the insulin resistance syndrome. Diabetes Care. 1999;22:1310-1317.
10. Plummer WA. Body weight in spontaneous myxedema. Trans Am Assoc Study Goiter.
11. Mariash CN. The thyroid and obesity revisited. Thyroid Today. 1998;19(3):1-9. 12. Hoogwerf BJ, Nuttall FQ. Long-term weight regulation in treated hyperthyroid and
hypothyroid subjects. Am J Med. 1984;76:963-970.
13. Pears J, Jung RT, Gunn A. Long-term weight changes in treated hyperthyroid and
hypothyroid patients. Scott Med J. 1990;35:180-182.
14. Ratzmann L, Hartmann K, Pflugradt K, et al. Changed body composition by increased body
fat content in experimentally hypothyroid rats. Endokrinologie. 1978;72:166-174.
15. Langdahl BL, Loft AGR, Eriksen EF, et al. Bone mass, bone turnover and body composition
in former hypothyroid patients receiving replacement therapy. Eur J Endocrinol. 1996;34:702-709.
16. Al-Adsani H, Hoffer LJ, Silva JE. Resting energy expenditure is sensitive to small dose
changes in patients on chronic thyroid hormone replacement. J Clin Endocrinol Metab. 1997;82:1118-1125.
17. Heymsfield SB, Wang Z-M. Human body composition: conceptual advances. In: A Angel, H
Anderson, et al., eds. Progress in Obesity Research: 7. London: John Libbey & Co.; 1996:245-257.
18. Khaleeli AA, Gohil K, McPhail G, et al. Muscle morphology and metabolism in hypothyroid
myopathy: effects of treatment. J Clin Pathol. 1983;36:519-526.
19. Boyages SC. The neuromuscular system and brain in hypothyroidism. In: LE Braverman,
RD Utiger, eds. Werner & Ingbar’s The Thyroid. A fundamental and clinical text. 8th Edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2000:803-810.
20. Hendel WH, Gotfredsen A, Andersen T, et al. Body composition during weight loss in obese
patients estimated by dual energy X-ray absorptiometry and by total body potassium. Int J Obes. 1996;20:1111-1119.
21. Pritchard JE, Nowson CA, Wark JD. A worksite program for overweight middle-aged men
achieves lesser weight loss with exercise than with dietary change. J Am Diet Ass. 1997;97:37-42.
22. Prior BM, Cureton KJ, Modlesky CM, et al. In vivo validation of whole body composition
estimates from dual-energy x-ray absorptiometry. J Appl Physiol. 1997;83:623-630.
23. Grodin JM, Siiteri PK, MacDonald PC. Source of estrogen production in postmenopausal
women. J Clin Endocrinol Metab. 1973;36:207-214.
24. Uzzan B, Campos J, Cucherat M, et al. Effects on bone mass of long term treatment with
thyroid hormones: a meta-analysis. J Clin Endocrinol Metab. 1996;81:4278-4289.
25. Lönn L, Stenlöf K, Ottosson M, et al. Body weight and body composition changes after
treatment of hyperthyroidism. J Clin Endocrinol Metab. 1998; 83:4269-4263.
26. Gómez Acotto C, Niepomniszcze H, Mautalen CA. Estimating body fat and lean tissue
distribution in hyperthyroidism by dual-energy X-ray absorptiometry. J Clin Densitometry. 2002;5:305-311.
27. Diamond T, Vine J, Smart R, et al. Thyrotoxic bone disease in women; a potentially
reversible disorder. Ann Intern Med. 1994;120:8-11.
Rivista Italiana di Ossigeno-Ozonoterapia 1: 149-153, 2002 A Novel Therapeutic Option for Chronic Fatigue Syndrome and Fibromyalgia Department of Surgery and Biomedical Engineering and *Department of Physiology, University of Siena; Italy Key words: chronic fatigue syndrome, fibromyalgia, ozone therapy SUMMARY - The aetiology of chronic fatigue syndrome (CFS) and fibromyalgia remains o
Wireless CodeSecure™ Keyfob Transmitter - User Guide Español Pulsador inalámbrico CodeSecure™ - Guía del Usuario Portuguese Comando Via Rádio CodeSecure™ - Manual de Utilizador Fig. 1 - MCT-234 ENGLISH 1. INTRODUCTION 3. TESTING AND MAINTENANCE The MCT-234 and MCT-234 NB (Narrow Band) are miniature 3.1 Testing a New Unit CodeSecure™ 4-button (4-function)
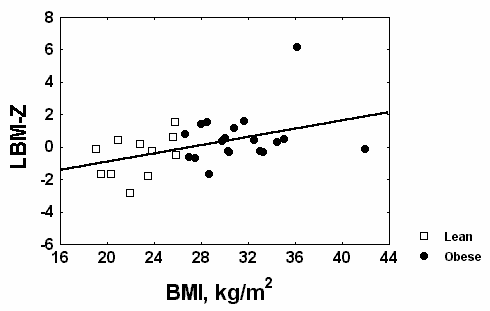
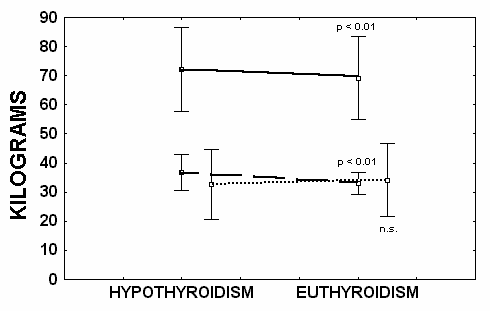 TABLE 4. Changes in Body Composition After Thyroid Hormone Replacement Therapy
TABLE 4. Changes in Body Composition After Thyroid Hormone Replacement Therapy 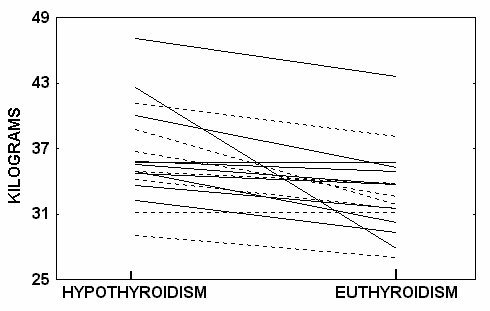 TABLE 5. Changes in the Fat Content (in kilograms) of the Trunk,
TABLE 5. Changes in the Fat Content (in kilograms) of the Trunk,